 C immitis a fungal organism acquired by inhalation.
C immitis a fungal organism acquired by inhalation.
Caused by soil fungi of the genus Coccidioides, divided into Coccidioides immitis, endemic to California, and Coccidioides posadasii, isolated outside of California.
Coccidioides is a dimorphic fungi that grows as a white mold at 77-86°F.
Coccidioides species reside in soil, infect humans via inhalation of airborne arthroconida (fungal spores).
Coccidioides have high tolerance for temperature, extremes, and soil pH, both of which may facilitate fungal survival.
Coccidioides growth in soil increases with heavy precipitation, and dispersion is facilitated when the soil dries.
The changes from dry and weight conditions, promote ideal conditions for fungal growth and infection transmission.
Fungus occurs naturally only in the Western Hemisphere an primarily in southwest U.S. and Mexico.
Fungus endemic in arid to semiarid climate, with hot summers, low altitude, alkaline soil and sparse vegetation-California and Arizona.
Climate change may expand the geographic regions at risk for coccidiomycosis but increasing temperatures and evaporative demand period.
These changes increase drought severity and soil drying in the American West with further increases anticipated pending on future global warming trajectory period.
Decreases in soil moisture and or increasingly wide or frequent swings between dry and wet conditions may promote environmental settings increasingly favorable to coccidioids growth and dispersion.
The fungal infection is endemic in semiarid portions of the western hemisphere.
About 150,000 cases occur annually in the U.S.
Diagnosis of coccicidioidmycosis is underdiagnosed with the actual number of coccicidioidmycosis cases is ten to 18 times higher than reported.
In 2023, the California Department of public health recorded 9210 cases of coccidiomycosis.
Presentation ranges from a self-limited respiratory illness to a life threatening process.
40% of patients infected with coccidioides develop symptoms.
Most commonly presents as a self limited upper respiratory tract infection in endemic areas.
Most infections are asymptomatic or cause minor respiratory disease.
Clinical disease, however, apparently develops in 1/3 of person is exposed to Coccidioides.
Patient with coccioides infection frequently experience, fever, cough, and shortness of breath.
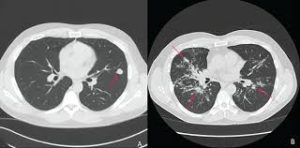
Chest x-ray imaging may demonstrate lobar, segmental, or multifocal consolidations, cavitation lesions and lung nodules.
Patients are often treated for community acquired pneumonia and coccidioidomycosis should be considered in patients, not improving with antibiotic treatment, or in those who have exposure to or reside in endemic areas.
Up to 50% of patients with pulmonary coccidiofomycosis have erythema nodosum, 25 to 30% have peripheral eosinophilia, and approximately 25% have arthralgias.
Patients generally develop a flu like syndrome with cough and fever.
It can manifest as lobar or segmental pneumonia with hilar adenopathy.
60% of people are asymptomatic.
Most infections are self-limited pulmonary infections acquired in the Southwestern US where the fungus is endemic.
About 75% of cases occur in Arizona in 25% in California.
Coccidioides hyphae produce barrel shaped arthroconidia.
Coccidioides arthroconidia in body tissues or fluids enlarge and develop into spherules containing endospores.
Most infections are caused by inhalation of spores.
60% of infected individuals remain asymptomatic.
Approximately 1 in 200 infected patients develop disseminated disease, which can develop multiple years after initial infection.
Inhaled organisms transform in the bronchioles into spherules and cause pulmonary infection.
Disseminated disease usually found in persons with altered cell immunity including patients with AIDS, Hodgkin’s disease and post solid organ transplant.
Pulmonary coccidiomycosis really progresses to acute respiratory distress syndrome, in which mortality may approach 100%.
Coccidioidal pneumonia most commonly presents with chest pain, cough and fever, while other symptoms include fatigue, dyspnea, headache, sore throat, and arthralgias.
Less commonly hemoptysis and erythema nodosum are present.
In immunocompetent individuals severe disseminated diseases is rare with an incidence of less than 1%.
Eosinophilia is noted in the peripheral blood in 25-30% of cases, and may help in differentiating coccidiomycosis pneumonia from a bacterial pneumonia.
Immune response to Coccidioides immunities is highly dependent to T cell lymphocytes.
Risk factors for severe or disseminated disease include racial heritage, pregnacy, or cell mediated immunodeficiency.
Corticosteroids have been found to increase the risk for coccidiomycosis but has been reported to be effective in treating patients with severe symptomatology.
Filipinos have the highest risk of dissemination, about 10-175 times the risk of Caucasians.
Blacks at significantly higher risk of developing disseminated disease.
Blacks have a 5 times higher risk of developing meningitis than whites and Filipinos have a 10 times higher risk.
Persons with group B blood type at higher risk for disseminated disease.
Patients with eosinophilia and high Ig levels have a worse prognosis.
Other groups with the increased risk for severe disease include pregnant women, infants, patients who have undergone thymectomy, patients with cancer, diabetes, or those immunocompromised.
Dissemination is typically to the skin with predilection to the nasolabial fold, bones, joints, meninges, and pleural space.
Mortality rate of non HIV infection hospitalized patients in California associated with a mortality rate of 8.2% ,while HIV infected patients had a mortality was24%(Flaherman ).
Disease outcomes depends on cellular immunity.
Heavy rains promote dispersion of agent by promoting growth in the soil and drought subsequently causes aerosolization of arthroconidia (Kolivras).
Outbreaks may be a result of atmospheric soil dispersion related to dust storms droughts, and earthquakes.
Occupational exposure in agricultural workers, excavators, military, archeologists are at highest risk for the development of this process.
Immunocompromised individuals including those with: AIDS/HIV, transplant recipients, patients receiving tumor necrosis factor inhibitors, pregnant women and patients with malignancy at high risk of this infection.
Diagnostic testing begins with serologic testing to detect Coccidia IgM and Ig””G antibodies with IgM detectable beginning at approximately three weeks after infection and complement fixation, which detects only IGG and results in positive findings by five weeks after infection.
A negative serologic test does not exclude coccidiomycosis, particularly in an immunocompromised patient.
Treatment of coccidioidomycosis with fluconazole is indicated for the meningeal form due to adequate CSF penetration and limited toxicity compared with amphotericin B.
Therapy is lifelong at doses of at least 400 mg daily.
Fluconazole is also effective for nonmeningeal forms of this disease, but itraconazole is preferred due to possible increased efficacy for skeletal infections.
More than 90% of patients with pulmonary coccidioidomycosis recovery without antifungals.
Recommendations for patients with pulmonary coccidioides infection who have had severe disease with comorrbidities, including diabetes should be treated with oral fluconazole for at least three months.
Patients with disseminated infection should typically be treated with oral azoles and should be referred to an infectious disease program.