 Cleft lip and cleft palate, also known as orofacial cleft.
Cleft lip and cleft palate, also known as orofacial cleft.
Cleft lip and palate occurs in about 1 to 2 per 1000 births in the developed world.
It caused about 4,000 deaths globally in 2010.
The highest prevalence rates for are reported for Native Americans and Asians.
Africans have the lowest prevalence rates.
Native Americans: 3.74/1000
Japanese: 0.82/1000 to 3.36/1000
Chinese: 1.45/1000 to 4.04/1000
Caucasians: 1.43/1000 to 1.86/1000
Latin Americans: 1.04/1000
Africans: 0.18/1000 to 1.67/1000
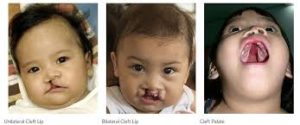
Refers to a group of conditions that includes cleft lip (CL), cleft palate (CP), and both together (CLP).
A cleft lip contains an opening in the upper lip that may extend into the nose.
A cleft lip opening may be on one side, both sides, or in the middle.
A cleft palate occurs when the roof of the mouth contains an opening into the nose.
Cleft lip and cleft palate disorders can result in feeding, speech and hearing problems, along with frequent ear infections.
Less than half the time left lip and cleft palate disorders are associated with other disorders.
Usually present at birth.
Cause usually unknown
Risk factors: Smoking during pregnancy, diabetes, obesity, older mother, certain medications like antiseizure agents.
Treatment is by surgery, speech therapy, dental care.
Frequency 1.5 per 1000 births.
The result of tissues of the face not joining properly during development.
A type of birth defect.
Surgery is often done in the first few months of life for cleft lip and before eighteen months for cleft palate.
Speech therapy and dental care may also be needed.
CL is about twice as common in males as females.
CP without CL is more common in females.
In 2013, it resulted in about 3,300 deaths globally.
If the cleft does not affect the palate it is referred to as cleft lip.
Cleft lip is formed in the top of the lip, and appears as a small gap or an indentation in the lip, a partial or incomplete cleft, or it continues into the nose as a complete cleft
Cleft lip can occur unilaterally or bilaterally.
It is due to the failure of fusion of the maxillary and medial nasal processes.
A mild form of a cleft lip is a microform cleft which appears as small as a little dent in the red part of the lip or look like a scar from the lip up to the nostril.
In some cases of microform cleft muscle tissue in the lip underneath the scar is affected and requires reconstructive surgery.
With cleft palate is a condition in which the two plates of the skull that form the hard palate are not completely joined.
The soft palate is in these cases cleft as well.
In most cases of cleft palate, cleft lip is also present.
Cleft palate occurs in about one in 700 live births worldwide.
Palate cleft can occur as complete involving the soft and hard palate, or incomplete, as a hole in the roof of the mouth, usually as a cleft soft palate.
The uvula is usually split when a cleft palate occurs.
It occurs due to the failure of fusion of the lateral palatine processes, the nasal septum, or the median palatine processes.
The opening in the roof of the mouth caused by a cleft connects the mouth directly to the inside of the nose, and is referred to as velopharyngeal inadequacy.
With velopharyngeal inadequacy air leaks into the nasal cavity resulting in a hypernasal voice resonance and nasal emissions while talking.
Velopharyngeal inadequacy can lead to speech articulation errors, and compensatory misarticulations and mispronunciations.
Velopharyngeal inadequacy treatments include: speech therapy, prosthetics, augmentation of the posterior pharyngeal wall, and lengthening of the palate.
Submucous cleft palate can occur, and is a cleft of the soft palate with a clinical triad of a bifid, or split, uvula, a furrow along the midline of the soft palate, and a notch in the back margin of the hard palate.
May impact an individual’s self-esteem, social skills and behavior.
Cleft palate can cause problems with feeding, ear disease, speech and socialization.
Individuals with cleft also face many middle ear infections which may eventually lead to hearing loss.
Babies with palatal clefts may have compromised hearing and therefore, are at risk for receptive language acquisition.
The lips and palate are both used in pronunciation, so individuals with cleft palate usually need the aid of a speech therapist.
The development of the face is susceptible to environmental and genetic factors.
During the first six to eight weeks of pregnancy, the shape of the embryo’s head is formed.
There are five primitive tissue lobes that develop in uterus:
one from the top of the head down towards the future upper lip, the Frontonasal Prominence.
two from the cheeks, which meet the first lobe to form the upper lip, the Maxillar Prominence.
two additional lobes grow from each side, which form the chin and lower lip-Mandibular Prominence.
If these tissues fail to meet, a gap appears where the tissues should have fused.
The birth defect reflects the locations and severity of fusion failures.
The upper lip is formed earlier than the palate.
The upper lip is formed from the first three lobes named a to c above.
Formation of the palate is the final step in joining the five embryonic facial lobes.
The formation of the palate involves the back portions of the lobes b and c.
The back portions, known as palatal shelves, grow towards each other until they fuse in the middle.
This fusion process is vulnerable to toxic substances, environmental pollutants, and nutritional imbalance.
Genetic factors contributing to cleft lip and cleft palate remain incomplete.
Clefts run in families, without an identifiable syndrome.
Genes involved include cleft lip and palate transmembrane protein 1 and GAD1,
There is an association between mutations in the HYAL2 gene and cleft lip and cleft palate formation.
The Van der Woude Syndrome is caused by a specific variation in the gene IRF6 that increases the occurrence of these deformities threefold.
Siderius X-linked mental retardation, is caused by mutations in the PHF8 gene, in addition to cleft lip or palate, symptoms include facial dysmorphism and mild mental retardation.
Cleft lip/palate may be present in many different chromosome disorders.
Many genes associated with syndromic cases of cleft lip/palate have been identified to contribute to the incidence of isolated cases of cleft lip/palate.
This includes sequence variants in the genes IRF6, PVRL1 and MSX1.
Fetal cleft lip and other congenital abnormalities have also been linked to maternal hypoxia, as caused by e.g. maternal smoking, maternal alcohol abuse or some forms of maternal hypertension treatment.
The diagnosis is made at the time of birth by physical examination.
It is possible to diagnose facial clefts in utero with ultrasonography.
Clefts can also affect other parts of the face, such as the eyes, ears, nose, cheeks, and forehead.
Within the first 2–3 months after birth, surgery is performed to close the cleft lip.
The preferred age for surgical repair is at approximately 10 weeks of age, so the child is at least 10 weeks of age; weighs at least 10 pounds, and has at least 10g hemoglobin.
The most common procedure to repair a cleft lip is the Millard procedure.
Often an incomplete cleft lip requires the same surgery as complete cleft.
Cleft palate can also be corrected by surgery, usually performed between 6 and 12 months.
Children with cleft palate typically speech difficulties, resulting directly from anatomical differences such as velopharyngeal inadequacy.
Velopharyngeal inadequacy refers to the inability of the soft palate to close the opening from the throat to the nasal cavity, which is necessary for many speech sounds.
Velopharyngeal inadequacy usually resolves after palate repair.
Hearing impairment is prevalent with cleft palate.
Because the tensor muscle fibers lack an anchor to function , the eustachian tubes do not open effectively.
When the air in the middle ear is absorbed by the mucous membrane, the negative pressure is not compensated, which results in the secretion of fluid into the middle ear space from the mucous membrane.
When this problem occurs typically have a conductive hearing loss primarily caused by this middle ear effusion.
A craniofacial team is routinely used to treat this condition.
There are dedicated cleft lip and palate programs.