The thoracic wall or chest wall is the boundary of the thoracic cavity.
The bony skeletal part of the thoracic wall is the rib cage, and the rest is made up of muscle, skin, and fasciae.
The chest wall has 10 layers:
skin (epidermis and dermis), superficial fascia, deep fascia and the invested extrinsic muscles from the upper limbs, intrinsic muscles associated with the ribs with three layers of intercostal muscles, endothoracic fascia and parietal pleura.
Extrinsic muscle layers vary according to the region of the chest wall.
The thoracic wall consists of a bony framework that is held together by twelve thoracic vertebrae posteriorly which give rise to ribs that encircle the lateral and anterior thoracic cavity.
The first nine ribs curve around the lateral thoracic wall and connect to the manubrium and sternum.
Ribs 10-12 are relatively short and attach to the costal margins of the ribs just above them.
Ribs 10-12, due to their short course, they do not reach the sternum.
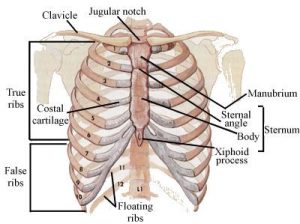
The first seven ribs are termed true ribs and attach to the manubrium and directly attach to the body of the sternum.
Ribs eight to ten only attach to the inferior part of sternum via the costal cartilages.
Ribs 11-12 are termed floating ribs because they do not attach directly to the sternum.
Ribs eight to ten are known as false ribs because they lack direct attachment to the sternum.
At the level of the spine, the ribs articulate with the costal facet of two opposing vertebrae.
The sternum defines the anterior chest wall.
The three separate bone segments of different size and shape that make up the sternum include 1) the thick manubrium, 2) long body of the sternum, and 3) the xiphoid process.
Anatomically, the manubrium is located at the level of thoracic vertebral bodies T3 and T4.
The manubrium is also the widest and thickest segment of the sternum.
The manubrium has the the suprasternal notch.
On either side of this notch, are the thick attachments from the clavicles.
A midline incision in the manubrium, allows access to the superior mediastinum, suprasternal goiter or thymus.
The sternal body is located at the level of vertebral bodies T5-T9.
To access the chest cavity, one can cut through the sternum with a mechanical saw.
The xiphoid process is a thin and very small bone, varying from two to five cm, and its shape is also variable.
The xiphoid may appear bifid, or oval.
It is curved inwards/outwards.
In younger individuals, the xiphoid is mostly cartilaginous but is nearly wholly ossified by age 40.
By age of 60 and over, the xiphoid is almost certainly completely calcified.
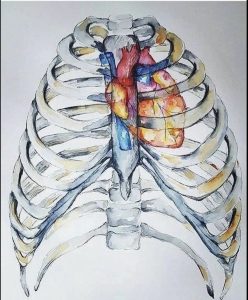
The thoracic cavity subdivides into three compartments; the mediastinum and two pleural cavities, one on each side.
The mediastinum, the median compartment, contains the heart and great vessels; whereas, the pleural cavities contain the lungs.
The thoracic cage protects the lungs and the heart as well as provide attachments for the muscles of the thorax, upper extremities, back, and the abdomen.
The thoracic cage communicates superiorly with the neck via the thoracic outlet and inferiorly separates the abdomen by the respiratory diaphragm.
The thoracic wall is bounded anteriorly by the sternum and costal cartilages; laterally by the ribs and intercostal spaces; posteriorly by the thoracic vertebrae and intervertebral discs; superiorly by the suprapleural membrane and inferiorly by the respiratory diaphragm.
Three arteries supply each intercostal space; the posterior intercostal artery and two branches of anterior intercostal arteries.
The intercostal blood vessels run along with the nerves between the internal intercostal muscle and innermost intercostal muscles in the costal groove.
They are arranged in order from superior to inferior: vein, artery, and nerve.
The posterior intercostal artery for first two intercostal spaces is fed from the superior intercostal artery from the costocervical trunk of the subclavian artery.
The remaining pair of posterior intercostal arteries from 3rd – 11th intercostal spaces and a pair of subcostal arteries emerge directly descending thoracic aorta.
The anterior intercostal arteries of 1st–6th intercostal spaces are branches of the internal thoracic artery which derive from the first portion of the subclavian artery.
The anterior intercostal arteries of 7th–9th intercostal spaces are branches of the musculophrenic artery which is a terminal tributary of the internal thoracic artery.
The anterior and posterior intercostal arteries anastomose laterally in the costal groove.
The corresponding posterior intercostal vein drains into azygos or hemiazygos veins and the corresponding anterior intercostal veins drain into internal thoracic or musculophrenic veins.
The lymphatics of the thoracic wall drains into parasternal lymph nodes and intercostal lymph nodes.
The parasternal lymph nodes and intercostal lymph nodes from the upper thorax drain into the bronchomediastinal trunk, whereas, the intercostal nodes from the lower thorax drains into the thoracic duct.
The thoracic wall is primarily innervated by the intercostal nerves, which are the anterior rami of spinal nerves of T1-T11 and the anterior ramus of T12 is a subcostal nerve.
Each intercostal nerve supplies a dermatome and a myotome.
There are three intercostal muscles; externally intercostal, internal intercostal and innermost intercostal muscles.
These muscles are present in the intercostal spaces and the intercostal nerves and blood vessels run between them.
The most superficial layer is the external intercostal muscle.
The internal intercostal muscle forms the intermediate layer.
The innermost intercostal muscle forms the deepest layer and is lined internally by the endothoracic fascia, which in turn is lined internally by the parietal pleura.
Median sternotomies are the most commonly performed osteotomy and a standard incision for thoracic and cardiac surgery.
The median sternotomy is a critical procedure in which the surgeon splits the sternum in the median plane to gain access to the heart, great vessels, as well as the lungs.
A flail chest, often caused by blunt chest trauma, results in multiple successive rib fractures.
The fractured ribs of the anterior and/or lateral chest wall move inward on inspiration and outward on expiration.
The vertical bone of the chest is the sternum, and it defines the anterior chest wall.
The three separate bone segments of different size and shape make up the sternum include: manubrium, body of the sternum, and the xiphoid process.
Anatomically, the manubrium is located at the level of thoracic vertebral bodies T3 and T4.
The manubrium is also the widest and thickest part of the sternum.
The suprasternal notch is at the top of the manubrium.
On either side of this notch, is the attachment from the clavicles.
The sternal body is located at the level of vertebral bodies T5-T9.
The xiphoid process a thin and small bone, varying from two to five cm, and of variable shape.
The xiphoid may appear bifid, or oval.
The xiphoid may curve inwards or outwards.
Early in life the xiphoid is mostly cartilaginous but is nearly wholly ossified by age 40.
By the age of 60 and over, the xiphoid is completely calcified.
The thoracic cavity is subdivided into three compartments; the mediastinum and two pleural cavities, one on each side.
The mediastinum is the median compartment containing the heart and great vessels.
The pleural cavities contain the lungs.
The thoracic cage is protective of the lungs and the heart.
The thoracic cage provides attachments for the muscles of the thorax, upper extremities, back, and the abdomen.
The thoracic cage communicates superiorly with the neck via the thoracic outlet and inferiorly separates the abdomen by the respiratory diaphragm.
The thoracic wall is bounded anteriorly by the sternum and costal cartilages.
The thoracic wall is bounded laterally by the ribs and intercostal spaces.
It is bounded posteriorly by the thoracic vertebrae and intervertebral discs, superiorly by the suprapleural membrane and inferiorly by the respiratory diaphragm.
Three arteries supply each intercostal space; the posterior intercostal artery and two branches of anterior intercostal arteries.
These intercostal blood vessels run along with the nerves between the internal intercostal muscle and innermost intercostal muscles in the costal groove.
They are arranged in order from superior to inferior: vein, artery, and nerve.
The thoracic wall is primarily innervated by the intercostal nerves.
The intercostal nerves are the anterior rami of spinal nerves of T1-T11 and the anterior ramus of T12 is a subcostal nerve.
Each intercostal nerve supplies a dermatome and a myotome.
There are three intercostal muscles; external, internal and innermost intercostal muscles.
These muscles are present in the intercostal spaces and the intercostal nerves and blood vessels run between them.
The most superficial muscle layer is the external intercostal muscle: extending posteriorly from the rib tubercle to the costochondral junction anteriorly
The internal intercostal muscle forms the intermediate layer, and it extends anteriorly from the sternum to the rib cage posteriorly where the muscle fibers are replaced the posterior intercostal membrane.
The innermost intercostal muscle forms the deepest layer and is lined internally by the endothoracic fascia, which in turn is lined internally by the parietal pleura.
Flail chest is a painful injury affecting the respiration, often caused by blunt chest trauma, resulting in multiple successive rib fractures.
With a flail chest the fractured ribs move inward on inspiration and outward on expiration and is paradoxical to normal chest movement.
A flail chest may be associated with pneumothorax and/or contusion of the heart and lung.
Flail chest management is through pain control, pulmonary toilet, and early ambulation.
It is not common to surgically repair the ribs in flail chest injury.
The sternum is a commonly used site for bone marrow aspiration because it possesses hematopoietic marrow.
Sternal puncture can pierce the structures related to the posterior surface of the manubrium such as the left brachiocephalic vein in the upper part and aortic arch in the lower part.
Thoracentesis can be performed to remove excess fluid from the thoracic cavity for both diagnostic or therapeutic purposes.
Pericardiocentesis is also a necessary procedure as it can be life-saving in a patient to remove excess fluid from the pericardial sac.
The thoracic outlet syndrome (TOS), refers to the compression of the neurovascular structures in the thoracic outlet, resulting in pain, numbness, weakness, muscle wasting, fatigue in the upper limbs as well as ischemia.
The brachial plexuses of nerves (C5, C6, C7, C8, and T1) and subclavian vessels, (artery and vein, are closely related to the first rib as well as the clavicle as they enter the upper limb.
These structures may be compressed between the scalene muscles and the first rib.
Pancoast tumors, as well as the presence of a rudimentary cervical rib, are among the potential causes of TOS.
The chest wall deformities, include pectus excavatum and pectus carinatum.