Cerebral amyloid angiopathy (CAA) is a condition where abnormal proteins (amyloid-beta) build up in the walls of the arteries in the brain.
This protein buildup weakens blood vessels, leading to a high risk of brain bleeding with a hemorrhagic stroke and cognitive decline.
Cerebral amyloid angiopathy (CAA) is a type of cerebrovascular disorder characterized by the accumulation of amyloid beta-peptide within the leptomeninges and small/medium-sized cerebral blood vessels.
Such amyloid deposition results in fragile vessels that may manifest in lobar intracerebral hemorrhages (ICH).
CAA is it is there second most common cause of spontaneous, intracerebral hemorrhage, characterized by deposition of misfolded beta amyloid in arteries in the cerebral cortex and leptomeninges.
It has been suggested that prion like transmissivity may occur with CAA.
Cerebral amyloid angiopathy, or CAA, is a condition where amyloid protein builds up in the walls of small blood vessels in the brain, making them fragile and prone to bleeding.
CAA is a common cause of lobar brain hemorrhage and can also be associated with cognitive decline, especially in older adults.
CAA can lead to small, often silent microbleeds or to larger intracerebral hemorrhages that cause sudden neurologic symptoms.
It may also cause transient focal neurologic episodes, seizures, headaches, or progressive memory and thinking problems.
Some cases are sporadic, while rare inherited forms can present earlier and more aggressively.
CAA is a key component an adverse responses to beta-amyloid (A𝜷) immunotherapy.
Manifestations: Brain Bleeds: Ranging from small, unnoticed microbleeds to larger, life-threatening strokes.
Cognitive Decline: Gradual loss of thinking abilities, memory problems, or dementia.
Amyloid Spells: Brief, recurring episodes of neurological symptoms that mimic mini-strokes, TIAs, migraines, or seizures.
CAA may also present with cognitive impairments, incidental microbleeds, hemosiderosis, inflammatory leukoencephalopathy, Alzheimer disease, or transient neurological symptoms.
CAA can induce an auto immune response.
Patients with CAA related inflammation typically have subacute encephalopathy or seizures, and sometimes focal neurologic deficits.
CAA can occur in certain familial syndromes or can sporadically.
Age: It is primarily a disease of aging, most commonly diagnosed in people over the age of 55.
The underlying cause is the deposition of amyloid-𝜷 in small- to medium-sized blood vessels.
While CAA is a distinct clinical entity, it shares overlapping protein pathology and frequently co-occurs with Alzheimer’s disease.
It is defined by deposition of the beta amyloid (A𝜷) peptide in walls of the small blood vessels of the brain and has a close with a relationship with the Abeta containing plaques of Alzheimer’s disease.
CAA contributes to an age related cognitive decline and affects central decisions about the use of anticoagulation therapy in stroke treatment and prevention in the use of anti-A/𝜷 immunotherapies for Alzheimer’s disease.
The A𝜷 fiber deposits that characterize CAA differ from those and Alzheimer’s disease, and that they are primary localized to cerebral blood vessel walls rather than brain tissue and are characterized by predominant of the shorter A𝜷 40 isoform rather than the longer A𝜷42 isoform.
A𝜷 deposits, surround arteriolar smooth muscle cell, and range from trace to full replacement of the arteriolar media and ultimately fragmentation of a vessel wall.
Cerebral hemorrhage occurs at the severe pathologic stage and likely the result of vascular remodeling that leads to replacement of the amyloid vessel wall segments with fiber and other plasma components, blood brain barrier leakage and accumulation of activated astrocyte of perivascular, microglia or macrophages.
The estimated prevalence based on postmortem neurological studies the prevalence of moderate to severe CAA is 23% in the general population and 47.5% among patients with the Alzheimer’s disease.
The tendency for the two diseases to overlap is related to shared pathophysiological mechanisms of.A𝜷 deposition, as well as partially shared predisposing risk factors, such as the presence of the e4 allele of APOE, the gene encoding apoliprotein E.
The prevalence of moderate to severe CAA is higher than the prevalence of hemorrhagic brain lesions suggesting brain hemorrhages develop in only a subgroup of patients with advanced CAA.
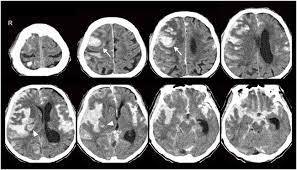
Diagnosis is typically made through advanced brain imaging. clinical, and pathological findings.
Neuroimaging evidence of multiple microhemorrhages or regions of cortical superficial siderosis may be seen.
CSF analysis may show mild pleocytosis and elevated protein levels, may but may also be normal.
MRI is one of the most important techniques used for diagnosis: Gradient-echo magnetic resonance imaging (MRI) demonstrates regions of low-signal blooming artifact caused by iron depositions left by old hemorrhages.
Brain biopsies are rarely utilized in the diagnosis of CAA.
Beta-amyloid immunostain or Congo red stains are techniques that can identify deposition of amyloid beta-peptide to help support the diagnosis of CAA.
Definitive diagnosis of CAA requires a postmortem examination of the brain.
MRI: Magnetic resonance imaging is the primary tool used to detect characteristic signs, such as multiple microbleeds concentrated in the outer layers of the brain (the cortex) and white matter changes.
MRI shows multiple hemorrhages or leptomeningeal blood products within or overlying the cerebral cortex.
There is no cure for CAA, and medical treatment focuses on preventing complications and managing symptoms.
Strict management of high blood pressure is crucial, as it lowers the stress on weakened blood vessels.
There must be caution with blood thinners, as these medications can significantly increase the risk of spontaneous brain bleeding.
Supportive Care: Cognitive symptoms and seizures are managed with targeted therapies.
Diagnosis is usually based on clinical features plus MRI findings such as lobar microbleeds and cortical superficial siderosis, with Boston criteria commonly used in practice.
Brain biopsy is rarely needed because imaging patterns are often enough to support the diagnosis.
Management
There is no cure, so treatment focuses on lowering the risk of further brain bleeding, especially by controlling blood pressure and avoiding medications that increase bleeding risk when possible.
Management of CAA cerebral hemorrhage is often based on presenting symptoms.
Acute management of patients with an ICH is similar to other spontaneous ICH.
Attention to blood pressure and intracranial pressure is essential.
Factors that are associated with a worse prognosis are intraventricular hemorrhage and age greater than equal to 75.
ICH associated with CAA is frequently recurrent.
CAA is important because it can mimic other neurologic disorders, and its bleeding risk affects decisions about anticoagulation, antithrombotic therapy, and stroke prevention.
Disease-modifying treatments are recently available.
The PROGRESS trial demonstrated a risk reduction of 77% for CAA-related ICH when blood pressure was controlled.
Pulsed cyclophosphamide or glucocorticoids result in sustained clinical improvement in inflammatory CAA.
Prognosis is dependent on CAA presenting features, with worse outcomes in patients with large hematomas and older age.
Individuals receiving red blood cell transfusions from donors who later develop multiple spontaneous intracerebral hemorrhages were significantly associated with increased risk of developing spontaneous intracerebral hemorrhage compared with receiving a transfusion from donors without subsequent intracerebral hemorrhage: suggesting a transfusion transmissible agent.
Cases of presenile CAA are caused by mutations in the amyloid precursor protein (APP) gene.
Patients with APOE epsilon 2 or epsilon 4 alleles seem to be at a greater risk for cranial hemorrhages than the general population.
Cerebral amyloid angiopathy is strongly age-dependent, with the prevalence of moderate to severe CAA increasing with age.
Sporadic CAA uncommonly affects individuals younger than 60 to 65
Sporadic CAA is rare in individual in their 50s.
CAA does not appear to have a predilection for gender.
There is a possible association between hypertension and CAA.
Cerebral amyloid angiopathy is usually asymptomatic.
When symptomatic, the most common clinical manifestation of CAA is spontaneous lobar hemorrhage.
The location and the size of the hemorrhage determines the clinical deficits as extending towards the ventricles may cause hemiplegia and decreased consciousness, while smaller hemorrhage may cause more focal deficits, headaches, or seizures.
Small cerebral amyloid angio patchy hemorrhages may be asymptomatic.
The hemorrhage location reflects the distribution of the amyloid-beta peptide, and favors cortical vessels.
The hemorrhages are more likely to occur in the posterior brain, as the cerebellum commonly contains vascular amyloid accumulation.
Cognitive impairment as a presenting symptom of amyloid angiopathy:
Gradual decline – microhemorrhages, lobar lacunas, microinfarcts, ischemic leukoencephalopathy
Step-wise decline – recurrent lobar hemorrhages
Rapidly progressive decline – cerebral amyloid angiopathy-related inflammation
The Boston criteria are a combination of clinical, pathological, and radiographic criteria that are used to assess the probability of CAA.
Definitive diagnoses can only be made through a postmortem examination of the brain.
Differential Diagnosis
Nontraumatic ICH includes:
Hemorrhagic tumor
Hemorrhagic transformation of an ischemic stroke
Lobar extension of a hypertensive putaminal hemorrhage
Arteriovenous malformation (AVM)
Hypertensive microangiopathy
Hemorrhagic metastases
Multiple cavernoma syndrome
Diffuse axonal injury
Radiation-induced vasculopathy
Neurocysticercosis
The prognosis of cerebral amyloid angiopathy is determined by the location and size of the ICH.
Unfavorable outcomes are associated with larger hematoma size and the age of the patient (≥75).
Favorable ICH outcomes are associated with sparing of the ventricles and a superficial location.
Mortality ranges from 10% to 30%, with the best prognosis seen in patients with increased consciousness and smaller hematomas.
CAA has a high hemorrhage recurrence risk, compared to a hypertensive hemorrhage:recurrence rates of around 21%.
CAA is commonly associated with both transient and cognitive neurological impairment, recurrent spells of numbness, paresthesias, and weakness.
Cerebral amyloid angiopathy intracerebral hemorrhage on anticoagulant therapy has a high mortality rate.
Alzheimer disease and CAA frequently coexist.
CAA has also been found to correlate with vascular dementia.
Complications
ICH
Transient neurologic symptoms
Cortical superficial siderosis
CAA-related inflammation
Cognitive impairment
CAA can occur in certain familial syndromes or sporadically.
Diagnosis is primarily made through a combination of clinical, pathological, and radiographic findings.
Prognosis is dependent on CAA presenting features, with worse outcomes in patients with large hematomas and older age.
Earliest recognizable pathological event in Alzheimer’s disease is cerebral amyloid-beta aggregation.
Cerebral amyloid-beta may be present 20 years before the onset of dementia and Alzheimer’s disease.
Cerebral amyloid can be assessed by cerebral spinal fluid biomarkers and by positron emission tomography.
Amyloid pathology in non-demented individuals is variable, from 10-70%.
Amyloid beta pathology is associated with age, APOE genotype and the presence of cognitive impairment.