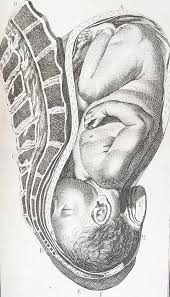
 Cephalic presentation, occurring in about 97% of deliveries, is the ideal “head-down” fetal position for childbirth, where the baby’s head enters the pelvis first, usually between 37-40 weeks gestation.
Cephalic presentation, occurring in about 97% of deliveries, is the ideal “head-down” fetal position for childbirth, where the baby’s head enters the pelvis first, usually between 37-40 weeks gestation.
Its prevalence increases progressively during the third trimester, rising from about 47% at 22 weeks to 94% by 36 weeks of gestation, after which the rate plateaus.
Cephalic presentation refers to where the head is the presenting part positioned toward the maternal pelvis, representing the normal and most common presentation at term.
It is the safest position for vaginal delivery, minimizing risks to the mother and baby.
Diagnosis is made via ultrasound or Leopold maneuvers via physical palpation.
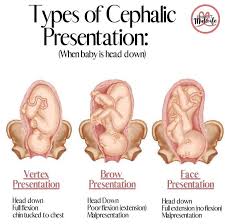
Vertex Presentation: The baby’s head is tucked chin-to-chest, presenting the smallest, top-back part of the head.
Vertex presentation represents the normal, well-flexed cephalic position.
Malpresentations demonstrate progressively increasing degrees of deflexion from vertex.
Military Presentation: The head is neither flexed nor extended, with the top of the head entering first.
Brow Presentation: The head is partially extended; the forehead (brow) is the leading part.
Face Presentation: The head is fully extended, causing the face to present first.
Spontaneous conversion from breech to cephalic presentation is unlikely after 36 weeks.
Timing: Most babies naturally turn to a head-down position/vertex by 36 weeks of pregnancy.
Cephalic presentation allows for a safer, more straightforward, and natural vaginal delivery with minimal complications.
While generally safe, malpositions like brow/face are rarely associated with cord prolapse can occur.
If the baby is not in a cephalic position by 36-37 weeks, an external cephalic version (ECV) may be attempted to turn the baby, or a C-section may be planned.
Diagnosis: Doctors use abdominal palpation (Leopold maneuvers) to feel for the hard, round head in the lower uterus, often confirming with ultrasound, particularly to check if the neck is extended.
Intrapartum ultrasound has proven more accurate than digital vaginal examination for diagnosing fetal position, malposition, and malpresentation during labor.
Management If the baby is not in a head-down position, techniques like prenatal yoga or staying upright may encourage turning.
If this fails, an external cephalic version (ECV) to manually turn the baby from the outside, which is usually done around 37 weeks.
Assessment of fetal presentation should ideally occur at 36 weeks’ gestation using ultrasound for confirmation.
Routine ultrasound examination at 35-37 weeks substantially reduces the risk of unexpected abnormal presentation during labor.
Malpresentations are recognized causes of failure to progress in labor and may require operative delivery.