 The cavernous sinus is one of the dural venous sinuses of the skull, creating a cavity called the lateral sellar compartment bordered by the temporal bone of the skull and the sphenoid bone, lateral to the sella turcica.
The cavernous sinus is one of the dural venous sinuses of the skull, creating a cavity called the lateral sellar compartment bordered by the temporal bone of the skull and the sphenoid bone, lateral to the sella turcica.
Cavernous sinus syndrome is a medical emergency, requiring prompt medical attention, diagnosis, and treatment.
The cavernous sinus is a network of veins that sit in a cavity on both sides of the sphenoidal bone and pituitary gland.
It is approximately 1 × 2 cm in size in an adult.
The carotid siphon of the internal carotid artery, and cranial nerves III, IV, V (branches V1 and V2) and VI all pass through this blood filled space.
Both sides of cavernous sinus is connected to each other via intercavernous sinuses.
The cavernous sinus lies in between the inner and outer layers of dura mater.
Above the cavernous sinus is the optic tract, optic chiasma, internal carotid artery.
Inferiorly to the cavernous sinus is the foramen lacerum, and the junction of the body and greater wing of sphenoid bone.
Medially to the cavernous sinus is the pituitary gland and sphenoidal air sinus.
Laterally to the cavernous sinus is the temporal lobe with uncus.
Anterior to the cavernous sinus is the superior orbital fissure, and the apex of the orbit.
Posterior to the cavernous sinus is the apex of petrous temporal bone.
The cavernous sinus receives blood from:
Superior and inferior ophthalmic veins
Sphenoparietal sinus
Superficial middle cerebral veins
Inferior cerebral veins
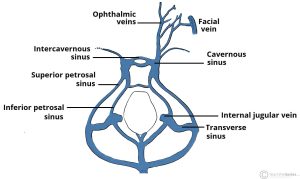
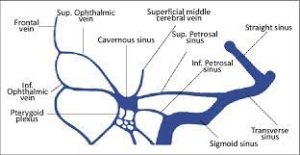
Cavernous sinus blood leaves via superior and inferior petrosal sinuses as well as via the emissary veins through the foramina of the skull.
Additionally, connections with the pterygoid plexus of veins via inferior ophthalmic vein, deep facial vein and emissary veins exist.
Some cranial nerves and their branches, also pass through the sinus: from superior to inferior
Oculomotor nerve
Trochlear nerve
Ophthalmic and maxillary branches of the trigeminal nerve
Abducens nerve
Internal carotid artery accompanied by the internal carotid plexus.
These nerves, with the exception of CN V2, pass through the cavernous sinus to enter the orbital apex through the superior orbital fissure.
The maxillary nerve, division V2 of the trigeminal nerve travels through the lower portion of the sinus and exits via the foramen rotundum.
The maxillary branch passes external to, but immediately adjacent to, the lateral wall of the sinus.
The optic nerve lies just above and outside the cavernous sinus.
The optic nerve superior and lateral to the pituitary gland on each side, and enters the orbital apex via the optic canal.
The cavernous sinus is a venous a venous sinus, that receives blood from the superior and inferior ophthalmic veins and from superficial cortical veins, and is connected to the basilar plexus of veins posteriorly.
The cavernous sinus drains by two larger channels, the superior and inferior petrosal sinuses, ultimately into the internal jugular vein via the sigmoid sinus, also draining with emissary vein to pterygoid plexus.
It is the only anatomic location in the body in which an artery travels completely through a venous structure.
If the internal carotid artery ruptures within the cavernous sinus, an arteriovenous fistula is created.
Abnormalities affecting the cavernous sinus may affect isolated nerves or all the nerves traversing through it.
The pituitary gland lies between the two paired cavernous sinuses.
Pituitary adenomas, sitting on the bony sella turcica, may expand in the direction of least resistance and eventually invade the cavernous sinus.
Cavernous sinus syndrome may result from mass effect of pituitary tumors and cause ophthalmoplegia=compression of the oculomotor nerve, trochlear nerve, and abducens nerve, ophthalmic sensory loss from compression of the ophthalmic nerve and maxillary sensory loss from compression of the maxillary nerve.
A complete lesion of the cavernous sinus disrupts CN III, IV, and VI, causing total ophthalmoplegia, usually accompanied by a fixed, dilated pupil.
Involvement of CN V causes sensory loss in these divisions of the trigeminal nerve.
Horner’s syndrome can also occur.
It is possible to get infections in the cavernous sinus from an external facial injury within the danger area of the face.
Thrombophlebitis clots the facial vein, pieces of the clomay break off and enter the cavernous sinus, forming a cavernous sinus thrombosis.
From there the infection may spread to the dural venous sinuses. Infections may also be introduced by facial lacerations and by bursting pimples in the areas drained by the facial vein.
Causes of cavernous sinus syndrome include : metastatic tumors, direct extension of nasopharyngeal tumours, meningioma, pituitary tumors or pituitary apoplexy, aneurysms of the intracavernous carotid artery, carotid-cavernous fistula, bacterial infection causing cavernous sinus thrombosis, aseptic cavernous sinus thrombosis, idiopathic granulomatous disease fungal infections.