Prevalence of primary cardiac tumors is approximately 0.02% , with 2 tumors per million autopsies.
Approximately 75% of sporadic myxomas occur in females, but the sexual predominance is less pronounced in familial atrial myxomas.
Myxomas occur from childhood to the elderly.
The mean age for sporadic cases is 56 years., while the mean age for familial cases is 25 years.
Most cases of atrial myxoma are sporadic, with unknown etiology.
Familial atrial myxomas have an autosomal dominant genetic transmission..]
It is associated with nonspecific symptoms, making early diagnosis difficult.
Dyspnea is the most common symptom.
May or may not produce characteristic findings on auscultation.
Two-dimensional echocardiography is the diagnostic procedure of choice.
Most atrial myxomas are benign and can be removed by surgical resection.
Account for 40-50% of primary cardiac tumors.
Approximately 90% are solitary and pedunculated.
75-85% of cases occur in the left atrium.
Up to 25% of cases are found in the right atrium.
Most cases are sporadic.
Approximately 10% are familial and are autosomally dominantly transmitted.
Multiple tumors occur in approximately 50% of familial cases.
Typically pedunculated and mobile lesions.
Familial cases are more frequently located in the ventricle, in up to 13% of cases.
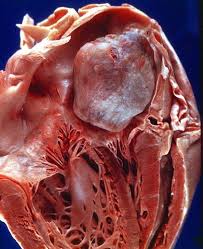
Myxomas appear as polypoid, round, or oval gelatinous lesions with a smooth or lobulated surface and are white, yellowish, or brown in appearance.
Vascular tumors.
The most common site of attachment is at the fossa ovalis in the left atrium.
Can also originate from the posterior atrial wall, the anterior atrial wall, or the atrial appendage.
Tumor mobility depends upon the extent of attachment to the interatrial septum and the length of the stalk.
Benign lesion, but local recurrence due to inadequate resection or malignant change may occur.
Occasionally, recur at a distant site because of intravascular tumor embolization.
Accounts for most cases of tumor embolism, and occurs in about 30-40% of patients.
The site of embolism is dependent upon whether the lesion is in the left or right atrium or if there is an intracardiac shunt present.
The risk of recurrence is higher in the familial myxoma syndrome.
Associated with sudden death in 15% patients, by coronary or systemic embolization or by obstruction of blood flow at the mitral or tricuspid valve.
Morbidity is related to symptoms produced by tumor embolism.
Symptoms are related to mechanical interference with cardiac function or embolization.
Systemic embolism is more common in polyploid tumors as compared to round lesions.
Symptoms vary from nonspecific and constitutional to sudden cardiac death.
Constitutional symptoms that include fever, weight loss, arthralgias, and Raynaud phenomenon are seen in 50% of patients.
20% of patients are asymptomatic and the lesion is discovered as an incidental finding.
Signs and symptoms of mitral stenosis, endocarditis, mitral regurgitation, and collagen vascular disease are similar to those of atrial myxoma.
Because of nonspecific symptoms a high index of suspicion is required for diagnosis.
Dyspnea on exertion is seen in 75% of patients with left sided heart failure and may progress to orthopnea, paroxysmal nocturnal dyspnea, and pulmonary edema.
Symptoms are caused by obstruction at the mitral valve orifice, and may may result in mitral regurgitation.
Symptoms of right-sided heart failure with fatigue and peripheral edema may occur.
Ascites is rare and it is more common in slowly growing right-sided tumors.
Dizziness and syncope occurs in approximately 20% of patients due to obstruction of the mitral valve., and such symptoms may be altered by the patients position.
Systemic or pulmonary embolization may occur from left- or right-sided tumors, respectively.
Left-sided systemic symptoms of embolization result in infarction or hemorrhage of distant organs.
Embolization to the central nervous system may result in transient ischemic attack, stroke, visual loss, or seizure activities.
Atrial myxoma with neurologic presentation is primarily an ischemic stroke in more than 80% of cases.
12% of left atrial myxomas with a neurological presentation manifest as seizures
Myxomas may induce cerebral aneurysms and metastases that can mimic vasculitis or endocarditis.
Right sided embolization can cause pulmonary embolism and infarction, and can result in pulmonary hypertension and cor pulmonale.
Presence of an intracardiac shunt via atrial septal defect or patent foramen ovale may result in a paradoxical embolism.
Hemoptysis due to pulmonary edema or infarction is observed in up to 15% of patients.
Associated with overproduction of interleukin-6.
Polyploid tumors also more frequently prolapse into the ventricle, which may result in destruction of the anulus or valve leaflets of the mitral or tricuspid valves.
Large lesions may be associated with atrial fibrillation.
Left atrial myxomas become symptomatic when they reach 70 g in volume, while right atrial myxomas grow to approximately twice that size before becoming symptomatic.
Lesions vary from 1-15 cm in diameter.
Myxomas produce growth factors and cytokines, including vascular endothelial growth factor, resulting in angiogenesis and tumor growth.
Has an increased expression of the inflammatory cytokine, interleukin-6.
Frequently causes emboli and immunologic manifestations.
Clinical findings include: elevated jugular venous pressures with prominent A waves, a loud S1 is caused by a delay in mitral valve closure due to the prolapse of the tumor into the mitral valve orifice, P2 may be delayed, or its intensity may be increased in the presence of pulmonary hypertension, an early diastolic sound reflecting the impact of the tumor against the endocardial wall, ref2242ed to as the tumor plop, may be present, an S3 or S4 may be audible, a diastolic atrial rumble may be heard if the tumor is obstructing the mitral valve, mitral regurgitation may cause a systolic murmur at the apex.
A right atrial tumor may cause a diastolic rumble or holosystolic murmur due to tricuspid regurgitation.
Clinically patients may have fever, cyanosis, clubbing, rash, or petechiae.
Familial myxoma may have a variety of features called syndrome myxoma or Carney syndrome: myxomas in breast, skin, thyroid gland, or neural tissue, lentigines , pigmented nevi, endocrine abnormalities, and cerebral aneurysms.
Carney syndrome is genetically heterogenous and is estimated to account for 7% of all atrial myxomas without any predilection for age or sex.
NAME syndrome: nevi, atrial myxoma, myxoid neurofibroma, and ephelides (freckles).
LAMB syndrome:lentigines, atrial myxoma, and blue nevi.
Patients with embolic stroke requires hospitalization.
No known medical treatment exists, but drug therapy is used only for congestive heart failure or cardiac arrhythmias.
The tumor must be removed surgically.
Some patients will also need their mitral valve replaced.
Complications are common and include: Arrhythmias, emboli, metastases, mitral valve blockage, stroke, cerebral aneurysms, and pulmonary edema.