 Atrial fibrillation (AF) and atrial flutter (AFL) are both supraventricular arrhythmias, but they differ in their mechanisms, ECG characteristics, and atrial activation patterns.
Atrial fibrillation (AF) and atrial flutter (AFL) are both supraventricular arrhythmias, but they differ in their mechanisms, ECG characteristics, and atrial activation patterns.
AF IS characterized by chaotic, disorganized atrial electrical activity with multiple reentrant wavelets, leading to an irregularly irregular ventricular response and loss of coordinated atrial contraction.
AFL is typically due to a single, organized macroreentrant circuit, which is most commonly around the tricuspid annulus in the right atrium (cavotricuspid isthmus-dependent flutter)—resulting in rapid, regular atrial activation.
ECG Findings:
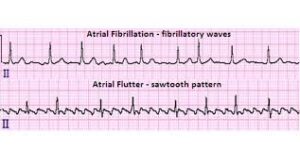
AF shows an absence of discrete P waves and an irregularly irregular ventricular rhythm.
AFL presents with regular, sawtooth flutter waves (especially in the inferior leads) and a more regular ventricular response, often with a fixed conduction ratio (e.g., 2:1 block).
Atrial Rate:
AF atrial rates are typically 300–500 bpm, but only a fraction of impulses conduct to the ventricles.
AFL atrial rates are usually 240–340 bpm, with a more predictable ventricular response depending on AV nodal conduction.
AF and AFL often coexist in the same patient and share similar risk factors and management strategies, including anticoagulation based on stroke risk.
AFL can be triggered by AF or antiarrhythmic therapy for AF, and ablation of typical AFL does not eliminate the risk of future AF.
AF is an irregular, disorganized arrhythmia, while AFL is a regular, organized macroreentrant rhythm—distinctions that are critical for diagnosis and management.