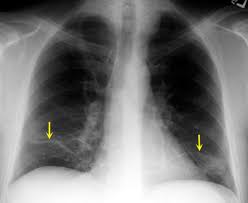
 Refers to incomplete expansion of the lung or the collapse of previously inflated lung, with areas of relatively airless pulmonary parenchyma.
Refers to incomplete expansion of the lung or the collapse of previously inflated lung, with areas of relatively airless pulmonary parenchyma.
It is the collapse or closure of lung tissue, leading to reduced or absent gas exchange in the affected areas.
It can occur due to various mechanisms, including airway obstruction (resorptive atelectasis), hypoventilation (passive atelectasis), external compression (compressive atelectasis), and increased surface tension (adhesive atelectasis).
Barotrauma is the most harmful aspect of mechanical ventilation: over-stretching of the airways and alveoli.
Surfactant is normally in activated and/or depleted continuously and must be continuously secreted to maintain low surface tension and prevent atelectasis.
Surfactant’s stimulus to secrete is the mechanical stress resulting from stretching type II pneumocytes.
The sigh recruits more surfactant.
Resorption atelectasis results from complete obstruction of an airway and the resorption of the oxygen trapped in the alveoli, without impairment of blood flow through the alveolar walls.
Resorption atelectasis caused primarily by excessive secretions or exudates in smaller bronchi and often related to asthma, chronic bronchitis, bronchiectasis and postoperative state and with aspiration of foreign bodies.
Can be caused by bronchial cancers.
Compression atelectasis occurs when the pleural cavity contains fluid, exudate, blood, tumor or air and compresses and compromises lung function.
Compression atelectasis most common in congestive heart failure when pleural effusions develop, and in malignancy associated with pleural effusions.
Compression atelectasis also occurs when the diaphragm is elevated with subphrenic abscess or with postoperative state with basilar atelectasis.
The mediastinum shifts way from the affected lung with compressive atelectasis.
With contraction atelectasis the presence of local or generalized fibrosis in the lung or pleura prevent full expansion of the lung.
Reduces oxygenation and increases risk of infection.
Reversible with re-expansion of the lung, except in atelectasis caused by contraction.
There is little evidence implicating atelectasis as a cause of fever.