 Benign cysts occur in the cerebrospinal axis in relation to the arachnoid membrane.
Benign cysts occur in the cerebrospinal axis in relation to the arachnoid membrane.
A cerebrospinal fluid covered by arachnoidal cells and collagen that may develop between the surface of the brain and the cranial base or on the arachnoid membrane, one of the three membranes that cover the brain and the spinal cord.
A congenital disorder, and most cases begin during infancy.
Seen in up to 1.1% of the population.
2:1 male:female distribution.
Only 20% of patients have symptoms.
Symptoms are usually from secondary hydrocephalus.
A study that looked at 2,536 healthy young males found a prevalence of 1.7% (95% CI 1.2 to 2.3%).
Rarely requires urgent medical attention.
Can be found on the brain, or on the spine.
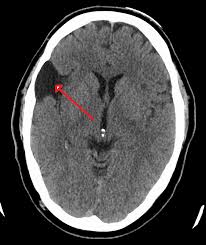
The most common locations for an arachnoid cyst: middle fossa and the posterior fossa (0.05% births).
The most common symptoms are nausea and vertigo.
Intracranial arachnoid cysts usually occur adjacent to the arachnoidal cistern.
Spinal arachnoid cysts may be extradural, intradural, or perineural and tend to present with signs and symptoms of a radiculopathy.
Classified as primary, that is, congenital) or secondary, acquired.
Can be relatively asymptomatic or present with insidious symptoms, often associated with delayed diagnosis.
Some patients never show symptoms,.
Symptoms vary by the size and location of the cysts.
Small cysts usually have no symptoms.
Do not communicate with the ventricular system of the brain.
Usually contain clear CSF.
May contain xanthochroid fluid.
Most are developmental abnormalities, but may be an acquired process.
Arachnoid cysts may be secondary to an associated malignancy, or from adhesions that occur with leptomeningitis, hemorrhage or surgery.
Accounts for approximately 1% of intracranial masses.
50%-60% occur in the middle cranial fossa.
Cysts in the middle cranial fossa more frequent in men and occur predominantly on the left side of the fossa.
Can occur in the spinal canal and can be in the subdural or epidural spaces.
Spinal lesions most commonly in the extramural dorsal thoracic region.
Intramural spinal arachnoid cysts can occur as a result of a congenital abnormality or from adhesions from previous trauma or infection.
Often found as an incidental finding on imaging studies.
Large cysts can cause enlargement of the head, particularly in children.
Clinical features include: headache, calvarial bulging and seizure activity.
Focal neurologic findings are unusual.
Cysts in the suprasellar region in children may be associated with the bobble-head doll syndrome, and cysts in the left middle cranial fossa have been associated with ADHD.
About 18% of patients with intracranial arachnoid cysts have non-specific headaches, and in 75% of these patients the cyst was in the temporal location.
A supratentorial arachnoid cyst can mimic a Ménière’s disease.
Frontal arachnoid cysts have been associated with depression.
Cysts on the left temporal lobe have been associated with psychosis, mood disorders and aggression.
Cyst on the right sylvian fissure may result in the onset of schizophrenia-like symptoms.
Cause is not known, but researchers suspect congenital malformations that arise from the unexplained splitting or tearing of the arachnoid membrane.
Some cases of hereditary disorders have been connected with arachnoid cysts.
Complications of arachnoid cysts can occur when a cyst is damaged by head trauma and can cause the fluid within a cyst to leak into other areas of the brain.
Blood vessels on the surface of a cyst may bleed into the cyst resulting in an intracystic hemorrhage, or bleed on the outside of the cyst resulting in a hematoma.
Bleeding complication collections can lead to increased intracranial pressure and brain compression symptoms.
Can occur secondary to Marfan syndrome, arachnoiditis, or agenesis of the corpus callosum.
Diagnosis is primarily by MRI.
Frequently an incidental finding on MRI scan.
In general, diagnosis requires the presence of symptoms to precipitate work-up, and many patients remain asymptomatic and undiagnosed,
Most cases are asymptomatic and do not require treatment.
A variety of procedures are used to decompress the cyst including a cerebral shunt placement with an internal shunt draining into the subdural compartment, or a cystoperitoneal shunt draining into the peritoneal cavity, a craniotomy with excision, drainage by needle aspiration or burr hole.
Most arachnoid cysts are asymptomatic, and require no treatment.
Leaving complicated cysts with expanding or hemorrhagic complications may cause permanent and neurological damage.
Surgical decompression of the cyst may improve neurological symptoms.
Treatment is surgical excision of the outer cyst membrane and cyst-peritoneal shunting.
Treatment with surgery is controversial, with some experts recommending treatment only for symptomatic patients.