The aorta is the largest artery in the human body, originating from the left ventricle of the heart and extending down to the abdomen.
The anatomy of the aorta can be divided into four main segments:
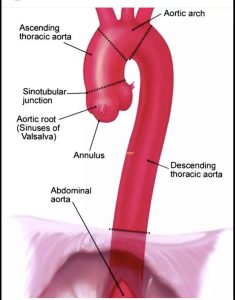
1. Ascending aorta: This is the first segment of the aorta, which originates from the left ventricle and ascends upward towards the neck.
It is about 5 cm long and has three main parts: the aortic root, aortic valve, and sinuses of Valsalva.
2. Aortic arch: The aortic arch is the second segment of the aorta, which bends over the top of the heart and extends towards the back of the body.
It has three main branches: brachiocephalic artery, left common carotid artery, and left subclavian artery.
3. Descending thoracic aorta: This is the third segment of the aorta, which runs down through the chest and delivers oxygenated blood to the thorax and upper abdominal organs.
It is about 20-25 cm long and has several branches, including intercostal arteries and bronchial arteries.
4. Abdominal aorta: The final segment of the aorta is the abdominal aorta, which runs through the abdomen and supplies oxygenated blood to the digestive organs, kidneys, and lower extremities.
It is about 12-15 cm long and has several branches, including the celiac artery, superior mesenteric artery, and renal arteries.
The wall has 3 layers: tunica intima, tunica media and adventitia.
May be associated with aortic dissection.
Acquired disease includes three categories of disease, aneurysmal, occlusive and aortic dissection.
Aortic stiffness in the presence hypertension, diabetes, and advanced age is implicated in the development of myocardial infarction, stroke and late onset CHF.
Aortic stiffness increases left ventricular afterload and promotes left ventricular hypertrophy.
Aortic stiffness associated with increased cardiovascular events.
Vascular stiffness increases with age and is a major risk factor for age-related morbidity and mortality.
Aortic compliance is an important buffer for ventricular contraction and maintains pulse pressure at low levels.
Aortic stiffening results in improper matching between the aorta diameter and blood flow and is associated with unfavorable alterations in pulsatile hemodynamics, including increased forward arterial pressure wave amplitude, which results in increases in pulse pressure.
Aortic wall stiffness is associated with elevated pulse wave velocity and premature wave reflection.
With increasing aortic stiffness there is an increase in pulsatile hemodynamic load which increases cardiac afterload, reduces diastolic coronary flow, damages the microcirculation, particularly in high flow organs such as the kidneys and brain.
Aortic stiffness correlates with age, hypertension, obesity, impaired glucose tolerance, and dyslipidemia.
Aortic stiffness is a major risk factor for all-cause mortality, cardiovascular disease, and hypertension
Higher aortic stiffness and forward to wave amplitude are associated with a higher risk of incident hypertension: this suggests that aortic stiffness is a precursor rather than the result of hypertension(Kaess BM et al).
Aortic wall stiffening may be related to vascular growth factor dysregulation, calcification, elastin degradation, information, and immune responses as well as the release of vasoactive factors by the endothelium.