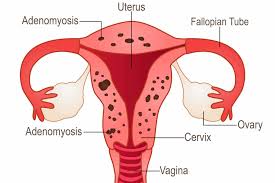
 Refers to a disorder in which endometrial glands and stroma are present focally or globally to the uterine musculature, resulting in hypertrophy of the surrounding myometrium.
Refers to a disorder in which endometrial glands and stroma are present focally or globally to the uterine musculature, resulting in hypertrophy of the surrounding myometrium.
Most patients are multiparous, in the fourth or fifth decades of life.
1/3 of cases are asymptomatic.
Women may present with heavy menstrual bleeding, irregular bleeding, dysmenorrhea, or dyspareunia.
Pathologic findings are related to: abnormal gene expression, increased angiogenesis, increased proliferation, decreased apoptosis, impaired choking expression, local estrogen production, resistance to progesterone, increased nerve density, and immunologic oxidative stress.
Diagnosis can bevassisted by transvaginal ultrasound and MRI, but definitive diagnosis rests on examination at hysterectomy.
Transvaginal ultrasound is associated with echogenic striations, myometrial cysts, globular uterine figuration, asymmetrical thickening of the myometrium, poor definition of the endometrial-myometrial interface.
Poor endometrial- myometrial interface findings has a sensitivity of 89% specificity of 89% for diagnosis.
Histologically there are irregularly shaped islands of endometrial glands and stroma in the endometrium.
These lesions are surrounded by hypertrophic and hyperplastic endometrium, further enlarging the uterus.
There are no laboratory confirming tests.
Dagnosis can be made by transvaginal ultrasound and MRI, with sensitivities ranging 70 to 80%.
MRI yields higher specific specificity than transvaginal ultrasound 83 to 92%, versus 74 to 81%.
Imaging studies frequently demonstrate an enlarged uterus, asymmetry of the myometrial thickness, diffusely abnormal/heterogeneous hypoechoic myometrial echotexture and poorly defined endometrial junction.
In contrast to fibroids there may be blood vessels traversing lesions.
No currently approved agents are available for treatment.
most measures use modalities to modulate estrogen and progesterone to suppress endometrial proliferation and diminish inflammatory cytokines and prostaglandins.
First line treatment for pain, bleeding and anemia is the levnorgestrel releasing intrauterine system.
Compared to oral medications, such as progesterone only or combined oral contraceptive pills, the levonorgestrel releasing intrauterine system provides a steady state of hormonal medication while providing contraceptive benefit, managing symptoms and avoiding hysterectomy in more than 2/3 of patients.
gonadotropin releasing hormone agonists can manage menstrual bleeding and pain but are associated with symptoms of hypo estrogenemia.
Uterine sparing techniques including uterine artery embolization for adenomyosis decreases heavy menstrual bleeding and dysmenorrhea, however 25% of patients will undergo subsequent hysterectomy for persistent symptoms.
Endometrial ablation diminishes bleeding and pain.
Excisional procedures such as adenomyomectomy, uterine wedge resection and hysteroscopic excision