 Accounts for 5-10% of all emergency department visits.
Accounts for 5-10% of all emergency department visits.
In 2015 healthcare expenditures for abdominal pain were estimated to be $10.2 billion.
Divided into visceral, parietal and referred abdominal pain is the chief complaint in abdominal pain in 50% of cases.
Visceral pain related to a viscus with tension, stretching or ischemia stimulating visceral pain fibers.
Visceral pain fibers are bilateral, unmyelinated, enter the spinal cord at multiple levels associated with dull pain, which is poorly localized and perceived to be in the midline.
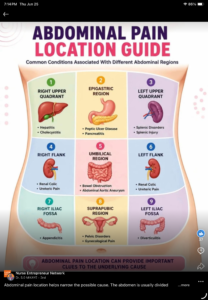
Midgut gastrointestinal structure, the small intestine, causes periumbilical pain.
Hindgut structure, large intestine causes lower abdominal pain.
Foregut structures, lower esophagus and stomach, cause discomfort the in the epigastrium.
Parietal pain arises from the parietal peritoneum as a result of ischemia, inflammation or stretching with transmission through myelinated afferent fibers to specific dorsal root ganglia on the same side and at the same dermatomal level as the origin of the pain.
Parietal pain is usually sharp, discrete, localized, intense and worsened by coughing and movement.
Referred pain felt in remote areas supplied by the same dermatome as the disease organ, resulting from shared central pathways for afferent neurons from different sites.(Example, abdominal pain from pneumonia with sharing of T9 dermatome).
Pain in the epigastric area indicates gastro-duodenal processes, right sub costal pain indicates hepatobiliary disease, and mid-lower abdominal pain indicates gynecologic disease among women ( Yammamoto, W et al ).
In young adults the differential diagnosis includes appendicitis, kidney stones, peptic ulcer disease, infectious enteritis, inflammatory bowel disease, cholecystitis, pancreatitis, referred pains, and in young women ectopic pregnancy, endometriosis, and pelvic inflammatory disease.
Diffuse pain may suggest ischemia, bowel obstruction, acute intermittent porphyria and diabetic ketoacidosis.
5% of patients with atypical coronary syndrome present with abdominal pain.
Flank pain is most commonly associated with renal disease, it may be seen with acute cholecystitis, pancreatitis and mesenteric ischemia.
In the evaluation of acute abdominal pain, early abdominal CT scanning provides better diagnostic accuracy then does standard supine abdominal and chest imaging, and less frequent misses unexpected and serious conditions.
CT of the abdomen in evaluating acute abdominal pain has 89% sensitivity and a 77% specificity in diagnosing serious conditions (Lameris W et al).
Administering opioid analgesic medications to adult and pediatric patients with acute undifferentiated abdominal pain is safe; no study has shown that analgesics adversely affect the accuracy of physical examination.