 Normothermic Regional Perfusion (NRP) is a specialized organ procurement technique used to restore oxygenated blood flow to a donor’s organs at normal body temperature after death has been declared by circulatory criteria.
Normothermic Regional Perfusion (NRP) is a specialized organ procurement technique used to restore oxygenated blood flow to a donor’s organs at normal body temperature after death has been declared by circulatory criteria.
Normothermic regional perfusion (NRP) is an advanced organ preservation technique that uses extracorporeal membrane oxygenation (ECMO) to provide in situ perfusion of donor organs with oxygenated blood at normothermic temperatures after declaration of death in donation after circulatory death (DCD) donors.
NRP is used during Donation after Circulatory Death (DCD) to minimize “warm ischemic time”—the period when organs are without oxygen—which significantly improves organ viability and transplant outcomes.
Declaration of Death: The donor is declared dead after their heart and lungs permanently stop functioning.
No-Touch Period: A “hands-off” period of typically 5 minutes is observed to ensure no spontaneous restart of the heart.
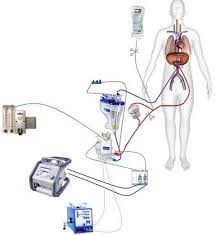
Circuit Initiation: insertion of cannulas and use an Extracorporeal Membrane Oxygenation (ECMO) machine to restart blood flow only in a specific region of the body.
Isolating the Brain: Critically, the blood vessels leading to the brain are clamped or ligated to ensure no blood reaches the head, preventing any possibility of “resuscitating” the donor’s neurological function.
Types of NRP
Abdominal (A-NRP): Only the abdominal cavity is perfused, typically to recover the liver and kidneys.
Thoracoabdominal (TA-NRP): Perfusion includes the chest, allowing the heart to begin beating again inside the donor’s body so surgeons can assess its function before procurement.
Benefits of NRP
Higher Organ Quality: Reduces rates of early graft failure and complications like ischemic cholangiopathy (bile duct damage) in livers.
Increased Utilization: Allows for the recovery of organs (especially hearts) that would traditionally be considered too damaged for transplant in standard DCD cases.
Allows surgeons to see the heart beating or the liver clearing lactate while still in the donor, confirming they are healthy enough for a recipient.
NRP is debated because it involves restarting circulation in a body recently declared dead based on the permanent cessation of circulation.
This technique rehabilitates ischemic injury incurred during the dying process and has become increasingly adopted with demonstrated improvements in organ utilization and transplant outcomes.
NRP is performed after death declaration by inserting cannulas into the arterial and venous circulation, occluding cerebral circulation to prevent brain perfusion, and initiating ECMO.
Abdominal NRP (A-NRP) limits perfusion to the abdominal cavity, targeting kidneys, liver, and pancreas while excluding the heart.
Thoracoabdominal NRP (TA-NRP) perfuses both thoracic and abdominal organs, allowing the heartbeat to be restored and enabling cardiac function assessment before procurement.
TA-NRP typically lasts 45 minutes to 2 hours to allow cardiac recovery from ischemia-reperfusion injury.
Evidence demonstrates superior outcomes with NRP compared to standard rapid recovery (SRR).
For liver transplantation, NRP is associated with complete elimination of ischemic cholangiopathy in some studies, while maintaining comparable patient and graft survival.
NRP reduced delayed graft function from 49.7% to 30.3%, shortened hospital stays, and improved overall graft and patient survival at 3 years.
Benefits were particularly pronounced in high-risk subgroups including elderly recipients or donors, high donor BMI, higher KDPI scores, and prolonged pre-transplant dialysis.
A UK study found NRP increased the odds of organ transplantation 3-fold for liver, 1.5-fold for kidney, and 1.6-fold for pancreas, with a mean of 3.3 organs transplanted per donor versus 2.6 without NRP.
For hearts, DCD transplants using NRP demonstrated comparable 1-year survival to traditional donation after brain death hearts.
By the end of 2023, nearly all 55 US organ procurement organizations had participated in NRP recoveries, with TA-NRP cases substantially outnumbering A-NRP cases (approximately two-thirds of all NRP procedures).
Heart transplant centers have been the primary drivers of NRP expansion.