 Tumor margin assessment is the evaluation of the edges of surgically removed tissue to determine if all cancer cells were successfully excised.
Tumor margin assessment is the evaluation of the edges of surgically removed tissue to determine if all cancer cells were successfully excised.
Tumor margins refer to the rim of normal tissue surrounding a resected tumor specimen, and their status is one of the most critical determinants of local recurrence risk and need for adjuvant therapy across virtually all solid tumor types.
It is a critical predictor of local recurrence and guides the need for additional treatments like re-excision surgery or radiation.
There is no universal definition of what constitutes an adequate margin — optimal width varies significantly by tumor type, anatomic site, histology, and use of adjuvant therapies.
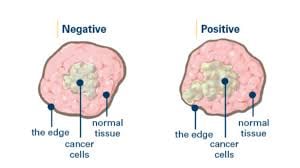
Pathologists classify margins based on the proximity of cancer cells to the inked edge of the specimen:
Margins are generally classified using the R classification system: R0 (microscopically negative margins), R1 (microscopically positive/involved margins), and R2 (grossly positive/residual tumor).
The specific definitions of “positive,” “close,” and “negative” vary by tumor type:
Negative (Clean): No cancer cells are found at the edge of the removed tissue.
Positive (Involved): Cancer cells extend to the edge (inked surface), suggesting some tumor remains in the patient.
Close: Cancer cells are very near the edge but do not touch it.
Definitions of “close” vary by cancer type and institution, often ranging from <1 mm to <5 mm.
Assessment can occur during surgery (intraoperative) or after surgery is complete (postoperative).
Pathology: Tissue is fixed in paraffin and examined days later for precise measurement.
Frozen Section | Rapid intraoperative analysis (20–30 mins).
It is essential for Mohs surgery but challenging in fatty tissues like the breast. | Touch Prep/Cytology | Specimen edges are touched to a slide to look for loose cancer cells.
While fast but cannot detect cancer hidden beneath the surface.
Imaging-Specimen X-ray Uses 2D or 3D (tomosynthesis) X-rays to check for microcalcifications or lesions.
Ultrasound | Real-time intraoperative visualization. Accurate for palpable masses but less sensitive for DCIS.
Breast Cancer: Guidelines for Ductal Carcinoma In Situ (DCIS) typically recommend a 2 mm clear margin, whereas invasive cancer often requires only “no ink on tumor”.
Breast cancer (invasive, stages I-II): A positive margin is defined as “ink on tumor”-any invasive cancer or DCIS cells touching the inked surface.
No wider margin is required for invasive cancer with whole-breast irradiation.
Mohs Surgery: Primarily for skin cancer, this technique allows for 100% margin evaluation in real-time, providing the lowest recurrence rates.
Margins are generally classified using the R classification system: R0 (microscopically negative margins), R1 (microscopically positive/involved margins), and R2 (grossly positive/residual tumor).
The specific definitions of “positive,” “close,” and “negative” vary by tumor type:
Head and neck SCC: NCCN defines positive as carcinoma at the inked edge, close as 1–4.9 mm, and clear/negative as ≥5 mm, though this traditional 5 mm threshold has been disputed.
Glottic cancers require only 1–2 mm, while oral cavity cancers require wider margins (gross 10–15 mm target).
Melanoma: Margins are determined by Breslow thickness — 0.5 cm for in situ, 1 cm for ≤1.0 mm (T1), and 2 cm for >2 mm (T3–T4). For T2 (1–2 mm), guidelines vary between 1–2 cm.
Soft tissue sarcoma: Minimum safe clearance is approximately 5 mm without adjuvant RT and 1 mm with adjuvant RT for non-infiltrative high-grade sarcomas.
For infiltrative subtypes ≥10 mm is advocated to minimize local recurrence.
Colorectal liver metastases: A ≥1 mm cancer-free margin is considered curative, though margins >1 cm may confer additional survival benefit.
Rectal cancer: The circumferential resection margin (CRM) is positive if tumor is ≤1 mm from the margin, and is a powerful predictor of local recurrence.
Early colorectal cancer (endoscopic resection): Traditionally, a submucosal margin.
Positive margins are consistently associated with a ≥2-fold increase in local recurrence across tumor types.
In breast cancer, this risk is not nullified by radiation boost, systemic therapy, or favorable tumor biology.
Breast cancer (invasive, stages I-II): A positive margin is defined as “ink on tumor” (any invasive cancer or DCIS cells touching the inked surface).
In head and neck cancer, positive margins are an indication for adjuvant chemoradiation.
Head and neck SCC: NCCN defines positive as carcinoma at the inked edge, close as 1–4.9 mm, and clear/negative as ≥5 mm, though this traditional 5 mm threshold has been disputed.
Importantly, revising an initially positive margin to negative (re-resection) is not equivalent to achieving a negative margin on the first attempt, as demonstrated in oral cavity cancer studies where re-resected margins did not reliably improve local control.
Margins can be assessed intraoperatively via frozen section (89–97% accuracy) or on final permanent sections.
Specimen-oriented radial (perpendicular) sectioning is preferred over en face shave biopsies, as it allows quantitative measurement of margin distance.
For skin cancers, Mohs micrographic surgery/PDEMA provides complete peripheral and deep margin assessment with superior cure rates.
Glottic cancers require only 1–2 mm, while oral cavity cancers require wider margins (gross 10–15 mm target).
Melanoma: Margins are determined by Breslow thickness — 0.5 cm for in situ, 1 cm for ≤1.0 mm (T1), and 2 cm for >2 mm (T3–T4).
For T2 (1–2 mm), guidelines vary between 1–2 cm.
Soft tissue sarcoma: Minimum safe clearance is approximately 5 mm without adjuvant RT and 1 mm with adjuvant RT for non-infiltrative high-grade sarcomas.
For infiltrative subtypes (myxofibrosarcoma, UPS), ≥10 mm is advocated to minimize local recurrence.
Colorectal liver metastases: A ≥1 mm cancer-free margin is considered curative, though margins >1 cm may confer additional survival benefit.
Rectal cancer: The circumferential resection margin (CRM) is positive if tumor is ≤1 mm from the margin, and is a powerful predictor of local recurrence.
Early colorectal cancer (endoscopic resection): Traditionally, a submucosal margin.
Positive margins are consistently associated with a ≥2-fold increase in local recurrence across tumor types.
In breast cancer, this risk is not nullified by radiation boost, systemic therapy, or favorable tumor biology.
In head and neck cancer, positive margins are an indication for adjuvant chemoradiation.
Importantly, revising an initially positive margin to negative (re-resection) is not equivalent to achieving a negative margin on the first attempt, as demonstrated in oral cavity cancer studies where re-resected margins did not reliably improve local control.
There is an exponential relationship between margin distance and local recurrence in oral cancer, showing that the greatest risk reduction occurs when moving from a positive margin to even 1 mm of clearance.
Margins can be assessed intraoperatively via frozen section (89–97% accuracy) or on final permanent sections.
Specimen-oriented radial/perpendicular sectioning is preferred over en face shave biopsies, as it allows quantitative measurement of margin distance.
For skin cancers, Mohs micrographic surgery/PDEMA provides complete peripheral and deep margin assessment with superior cure rates.