 Papillary renal cell carcinoma (PRCC) is a malignant tumor originating from renal tubular epithelial cells of the kidney, which comprises approximately 10-15% of all kidney neoplasms.
Papillary renal cell carcinoma (PRCC) is a malignant tumor originating from renal tubular epithelial cells of the kidney, which comprises approximately 10-15% of all kidney neoplasms.
It is estimated that the incidence of PRCC will rise to 3,500 to 5,000 cases annually.
PRCC is more prevalent among men than women, while the reported sex ratio (M: F) varies from 1.8:1 to 3.8:1.
African or Afro-Caribbean ancestry tend to have higher chances of being diagnosed with PRCC.
PRCC is more common in the Non-Hispanic Black population (38.9%) when compared to other races – Asian American (18.0%), Non-Hispanic White (13.2%), and Hispanic White populations (6.1%).
A malignant epithelial tumor of the kidney characterized by the presence of papillary or tubulopapillary architecture.
It is the second most common subtype of renal cell carcinoma. accounting for approximately 10–20% of cases.
Based on its morphological features, PRCC can be classified into two main subtypes, which are type 1 (basophilic) and type 2 (eosinophilic).
Most cases of PRCC are discovered incidentally without showing specific signs or symptoms of cancer.
In advanced stages, hematuria, flank pain, and an abdominal mass are the three major manifestations.
Risk factors identified to affect PRCC development, such as genetic mutations, kidney-related disease, environmental and lifestyle risk factors.
Molecularly, PRCC often harbors gains of chromosomes 7 and 17, loss of the Y chromosome, and up to 15% have MET gene alterations, particularly in low-grade tumors. High-grade tumors may also show these chromosomal changes but are more heterogeneous genetically.
Hereditary forms, such as those associated with germline MET mutations or FH deficiency (as in hereditary leiomyomatosis and renal cell cancer syndrome), are recognized and have distinct clinical implications.
Type 1 PRCC is mainly caused by MET gene mutation while type 2 PRCC is associated with several different genetic pathways.
PRCC is detectable through computed tomography (CT) scans or magnetic resonance imaging (MRI), which commonly present a small homogeneous hyposvascular tumor.
Nephrectomy or partial nephrectomy is usually recommended for PRCC treatment, often accompanied with several targeted molecular therapies to inhibit metastatic spread.
PRCC patients are predominantly male with a mean age of 52–66 years.
When compared to conventional clear cell renal cell carcinoma (RCC), the prognosis of non-metastatic PRCC is more favorable, whereas a relatively worse outcome was reported in patients with metastatic disease.
Globally, the incidence of PRCC ranges between 3,500 and 5,000 cases, while it greatly varies depending on gender, age, and race/ethnicity.
Treatment Nephrectomy, partial nephretocmy, targeted molecular therapy
Prognosis 82-90% for five-year survival rate
Type 1 PRCC, caused by a genetic predisposition of hereditary papillary renal cancer syndrome, compromises approximately 25% of all PRCCs.
Immunochemistry profile has a strong CK7 and alpha-methyl acyl-CoA racemase (AMACR) expression at most focal CA-IX expression.
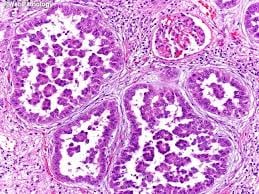
Histologically, its epithelium is composed of relatively small-sized simple cuboidal cells lined in a single layer, and are characterized by scarce basophilic cytoplasm.
A compact papillary architecture is often observed, and other morphological characteristics include intracellular hemosiderin and foamy macrophages placed inside of papillary fibrovascular cores or psammoma bodies.
The nuclei of type 1 PRCC belong to grade 1-2 of the Fuhrman system.
Small basophilic cells with scarce cytoplasm as a single layer of cells are surrounding the basal membrane.
Foamy macrophages are inside of papillary fibrovascular cores.
Type 2 PRCC cells containing abundant eosinophilic granular cytoplasm with prominent nucleoli.
Type 2 PRCC’s account for 25% of PRCCs, and is the pathological subtype that is most commonly associated with hereditary leiomyomatosis and renal cell carcinoma (HLRCC) syndrome.
When compared to type 1 PRCC it shows more variation in protein expression mostly by loss of CK7, and its gross examination shows papillae covered by large cells abundant in eosinophilic cytoplasm.
Foamy macrophages and psammoma bodies are less common in case of type 2, and the majority of type 2 PRCC has high Fuhrman grade nuclei with prominent nucleoli.
PRCC is often asymptomatic and undetectable, and the majority of cases are incidentally diagnosed during the radiological workup of unrelated diseases.
Its clinical manifestations are similar to those of clear cell RCC: classical triad of renal cell carcinoma with hematuria, flank pain and palpable abdominal mass seen only 6-10% of patients, or even nonspecific symptoms including fatigue, weight loss, fever, and anorexia.
Metastasis occur most frequently in the lungs followed by bone and the brain, exhibiting a wide range of symptoms including bone pain to a persistent cough.
Possible risk factors have been identified that contribute to PRCC development: genetic mutations, hereditary syndrome, renal injuries, and lifestyle factors.
Germline mutation of c-MET oncogene and fumarate hydratase gene elevates the risk of type 1 and type 2 PRCC respectively through distinct signaling pathways.
Patients with hereditary papillary renal cancer syndrome showed a greater risk of type 1 PRCC, whereas those with hereditary leiomyomatosis and renal cell cancer (HLRCC) syndrome have an increased risk of type 2 PRCC.
Patients who experience chronic kidney diseases or acute kidney injury exhibited a higher incidence of PRCC, and other risk factors such as smoking, obesity, and high blood pressure can influence the pathogenesis of PRCC.
Type 1 PRCC is caused by a genetic mutation or a gain in chromosome 7 where the MET gene is positioned.
The genetic mutation or a gain in chromosome 7 results in the promotion of oncogenic pathways in renal epithelial cells.
The MET gene is upregulated for renal tissue repair and regeneration by encoding the receptor tyrosine kinase c-MET of hepatocyte growth factor.
The activation of the oncogenic pathway in the MET gene manifests as invasion, anti-apoptosis, angiogenesis, and metastasis.
Type 2 PRCC is associated with irregularity of several signaling pathways, which includes CDKN2A silencing, mutation in chromatin-modifying genes, and a GpG island methylator phenotype (CIMP).
CDKN2A is a tumor suppressor gene, while loss of its expression results in enhanced tumorigenesis and metastasis.
Diagnosis:
Imaging with computed tomography (CT) and magnetic resonance imaging (MRI) is known as the best option for diagnosing papillary renal tumors.
Contrast-enhanced computed tomography (CT) is most commonly used to identify the subtypes of RCC.
PRCC can be differentiated from other types of RCC due to its distinguishing features, displaying a small hypovascular renal tumor on T2 weighted images.
PRCC tends to appear homogeneous while clear cell RCC is likely to be in a heterogeneous form when the tumor is less than 3 cm in diameter.
In cases of tumors larger than 3 cm in diameter, PRCC is generally heterogeneous with areas of necrosis and hemorrhage compared to chromophobe RCC.
Solid, small PRCC tumors (<3 cm in diameter) are more easily viewed on nephrographic, excretory phase images rather than on unenhanced, corticomedullary phase images.
As some renal tumors do not enhance significantly on CT, MRI examination is required to be performed with more sensitive contrast enhancement.
On MRI, the distinct features of PRCC are fibrous capsules and homogeneously low single intensity on both T1- and T2-weighted images.
Specifically, PRCC exhibits hypointensity due to its dense collagenous matrix or deposition of calcium and hemosiderin within the tumor.
Such visual features help PRCC to be differentiated from clear cell RCC, which has heterogeneously higher single intensity shown on T2-weighted images.
PRCC displays the smallest tumor-to-cortex enhancement at corticomedullary and nephrographic phases when juxtaposed with clear cell and chromophobe RCCs.
Treatment:
First-line treatment for metastatic PRCC has not been standardized.
Similar treatment approaches for clear cell RCC have been used for PRCC.
Nephrectomy or nephron-sharing partial nephrectomy is widely recommended to reduce the risk of metastasis by eliminating all or part of the kidney.
Surgery procedures for PRCC depend on the patient’s status and are very similar to procedures performed on RCC patients.
Tyrosine kinase inhibitors (TKIs) and mammalian target of rapamycin (mTOR) inhibitors are effective in inhibiting angiogenesis, blocking growth and suppressing spread of the tumor.
Sunitinib, sorafenib, and axitinib are TKIs with anti-vascular endothelial growth factor (VEGF), which inhibit cellular signaling by targeting multiple receptor tyrosine kinase.
Everolimus and temsirolimus are used in deregulating the mTOR pathway.
Specifically, mTOR inhibitors have crucial roles in regulating cell growth, cell proliferation and metabolism of highly active tumor cells.
Other targeted agents such as MET inhibitors, epidermal growth factor receptor (EGFR) inhibitors, and monoclonal antibodies, are also promising treatment approaches for PRCC.
Immunotherapy and targeted therapies have demonstrated efficacy in patients with papillary renal cell carcinoma.
The five-year survival rate of PRCC has been reported as 82-90%, which is slightly higher than that of other kidney cancers.
The reduced survival rate is positively correlated to high nuclear grade and stage, vascular invasion, DNA aneuploidy.
Patients with type 1 PRCC have significantly improved survival rates than those with type 2, because of its lower TNM stage with a well-encapsulated tumor.
Compared to other common types of RCC, PRCC exhibits a relatively lower risk of tumor recurrence and cancer-related death after nephrectomy.
The cancer-specific survival rate at five years following surgery with PRCC has reached up to 91%, while clear cell RCC and chromophobe RCC were 72% and 88%, respectively.