 The erector spinae plane (ESP) block is a regional anesthesia technique
used to manage pain for various thoracic, abdominal, and some lower extremity surgeries and conditions.
The erector spinae plane (ESP) block is a regional anesthesia technique
used to manage pain for various thoracic, abdominal, and some lower extremity surgeries and conditions.
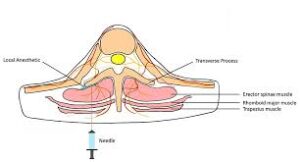
The erector spinae plane block (ESPB) is an ultrasound-guided regional anesthesia technique in which local anesthetic is injected into the fascial plane deep to the erector spinae muscle, adjacent to the transverse process of the vertebra.
The erector spinae muscles (iliocostalis, longissimus, and spinalis) run bilaterally along the spine from the skull to the sacrum.
The ESP block involves injecting a local anesthetic into the fascial plane deep to the erector spinae muscle and superficial to the transverse processes of the vertebrae.
This technique blocks the dorsal and ventral rami of spinal nerves, often producing a multi-dermatomal sensory block across the thoracic and abdominal walls.
The local anesthetic can diffuse both cranially and caudally, and sometimes anteriorly into the paravertebral space, contributing to extensive sensory coverage and visceral analgesia.
This block provides analgesia by spreading the anesthetic cranio-caudally and medially to affect the dorsal and ventral rami of the spinal nerves, and sometimes the paravertebral space, resulting in both somatic and visceral pain relief.
It is used for acute perioperative pain in thoracic, abdominal, breast, and spine surgeries, as well as for chronic pain and trauma.
ESPB is also being explored for analgesia in upper and lower limb procedures, with the advantage of sparing motor function.
It is usually performed between T5–T7, but can be used at other levels.
The block can cover multiple dermatomes, with a single injection at the thoracic level typically providing sensory blockade over 8–11 dermatomes.
Ultrasound guidance is used to identify the erector spinae muscle over the transverse process.
ESPB is considered technically simple, safe, and less invasive compared to traditional thoracic epidural or paravertebral blocks, with a lower risk of neurovascular or pleural injury.
The Tuohy needle is advanced under ultrasound guidance through the muscles until it contacts the transverse process, then local anesthetic is injected, often in 5 mL increments with total volumes of 20–30 mL.
Catheters may be placed for continuous infusion when prolonged analgesia is needed.
The erector spinae plane (ESP) block Is effective for thoracotomies, laparoscopic abdominal surgeries, ventral hernia repairs, rib fractures, and spine surgery.
The erector spinae plane (ESP) block Is associated with improved pain control, reduced opioid use, better lung function preservation, and enhanced recovery after thoracic surgery.
It has a favorable safety profile and is less technically challenging compared to some traditional blocks, such as thoracic epidural or paravertebral blocks.