
 The stellate ganglion, or cervicothoracic ganglion, is a sympathetic ganglion formed by the fusion of the inferior cervical ganglion and the first thoracic superior thoracic sympathetic ganglion, which is present in 80% of individuals.
The stellate ganglion, or cervicothoracic ganglion, is a sympathetic ganglion formed by the fusion of the inferior cervical ganglion and the first thoracic superior thoracic sympathetic ganglion, which is present in 80% of individuals.
Sometimes, the second and the third thoracic ganglia are included in this fusion.
The stellate ganglion is polygonal in shape and is relatively big (10–12 × 8–20 mm) compared to the much smaller thoracic, lumbar, and sacral ganglia.
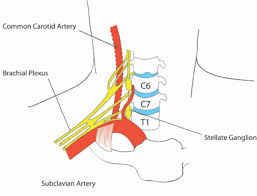
Stellate ganglion is located at the level of C7, anterior to the transverse process of C7 and the neck of the first rib, superior to the cervical pleura and just below the subclavian artery.
The stellate ganglion lies in front of the neck of the first rib, and posterior to the common carotid artery.
The stellate ganglia may be cut in order to decrease the symptoms exhibited by Raynaud’s phenomenon and hyperhydrosis of the hands.
Injection of local anesthetics near the stellate ganglion can sometimes mitigate sympathetically mediated pain symptoms such as complex regional pain syndrome type I (reflex sympathetic dystrophy), and symptoms associated with alterations in arousal and reactivity of PTSD.
Injection is often given near the anterior tubercle of transverse process of C6, due to this being an important landmark lateral to the cricoid cartilage.
It is thought that anesthetic is spread along the paravertebral muscles to the stellate ganglion.
Stellate ganglion block has potential as a means of reducing the number of hot flashes and night awakenings suffered by breast cancer survivors and women experiencing severe symptoms of menopause.
Stellate ganglion blocks have been used to treat PTSD.
Nerve fibers from the stellate ganglion go up the superior cervical sympathetic chain and into the pterygopalatine ganglion (SPG).
SPG blocks have been shown to reduce anxiety, headaches, migraines, cancer pain and other disorders.
Self-administration of SPG blocks (SASPGB) is a method of delivering sphenopalatine blockade and indirect stellate ganglion blockade.
Complications associated with a stellate ganglion block include Horner’s syndrome, accidental intra-arterial or intravenous injection, difficulty swallowing, vocal cord paralysis, epidural spread of local anaesthetic, and pneumothorax.
Left stellectomy is a treatment strategy in prolonged QT syndrome because activity of the stellate ganglia drives prolonged QT, and is only offered to patients who are already on a beta blocker and experience frequent shocks from an implantable cardioverter-defibrillator (ICD), because stellectomy causes Horner’s syndrome.
Stellate ganglion nerve block can also be used as a treatment for refractory ventricular tachycardia.