Scheuermann’s disease is a self-limiting skeletal disorder of childhood: the vertebrae grow unevenly with respect to the sagittal plane, the posterior angle is often greater than the anterior.
Frequency 5% (range 0.4% – 8%).
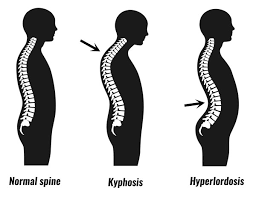
This uneven growth results in the wedging shape of the vertebrae, causing kyphosis.
It is considered to be a form of juvenile osteochondrosis of the spine.
Its cause is not currently known.
It is found mostly in teenagers and presents a significantly worse deformity than postural kyphosis.
Usual onset in adolescence.
More common in males.
Patients suffering with Scheuermann’s kyphosis cannot consciously correct their posture.
The apex of the spinal curvature is located in the thoracic vertebrae, and is quite rigid.
The process for causes lower and mid-level back and neck pain, which can be severe and disabling.
Patients may feel pain at the apex of the curve, which is aggravated by physical activity and by periods of standing or sitting.
In addition to the pain, many sufferers of the disorder have loss of vertebral height, and depending on where the apex of the curve is, may have a visual hunchback or roundback.
Curvature in the lower thoracic region may cause more pain, whereas curves in the upper region present a more visual deformity.
The seventh and tenth thoracic vertebrae are most commonly affected. In Scheuermann’s kyphosis, vertebrae are irregular, often herniated, and wedge-shaped over at least three adjacent levels.
In very serious cases it may cause internal problems and spinal cord damage, but these cases are extremely rare.
The curvature of the back decreases height, thus putting pressure on internal organs, wearing them out more quickly than the natural aging process.
The degree of thoracic kyphosis among Scheuermann’s patients is not related to back pain, quality of life, or general health.
Many patients with Scheuermann’s disease often have an excessive lordotic curve in the lumbar spine, compensating for the kyphotic curve above.
Many individuals with Scheuermann’s disease have very large lung capacities.
Men often have broad, barrel chests, and most people have forced vital capacity (FVC) scores above average.
Often patients with Scheuermann’s disease have tight hamstrings, possibly related to the body compensating for excessive spinal curvature.
In addition to the common lordosis, 20–30% of patients with Scheuermann’s disease also have scoliosis, though most cases are negligible.
In serious cases, the combination is classified as a separate condition known as kyphoscoliosis.
For unknown reasons patients with Scheurmann’s disease are prone to having a lower than average bone density.
Diagnosis is typically by medical imaging.
Scheuermann’s disease is self-limiting after growth is complete.
The process generally runs its course and never presents further complication, however, once the patient is fully grown, the bones will maintain the deformity.
Options are available to correct kyphosis while the spine is still growing, and aim to prevent it from worsening.
Physical therapy and/or back braces can help reverse or stop the kyphosis before it does become severe.
Physiotherapy and bracing are the first-line treatments for this condition.
Surgery is usually considered a last resort for patients: spinal fusion and hardware instrumentation.
There are two primary surgical techniques to correct kyphosis: posterior-only fusion: trends are favoring posterior-only fusion.