 Pituitary apoplexy (PA) refers to bleeding into or impaired blood supply of the pituitary gland.
Pituitary apoplexy (PA) refers to bleeding into or impaired blood supply of the pituitary gland.
This usually occurs in the presence of a tumor of the pituitary.
Pituitary apoplexy is rare.
In people with a known pituitary tumor, only 0.6–10% experience apoplexy.
The risk of PA is higher in larger tumors.
Expect 18 cases of pituitary apoplexy per one million people every year.
The average age at onset is 50.
Men are affected more commonly than women, with a male-to-female ratio of 1.6.
The majority of the underlying tumors are nonsecretory tumors, which explains why the tumor has often gone undetected prior to an episode of apoplexy.
In 80% of cases a pituitary tumor was undiagnosed previously.
The most common initial symptom is a sudden headache.
Often there is associated with a visual field defect or double vision caused by compression of nerves surrounding the gland.
The process is often followed by acute symptoms due to lack of secretion of essential hormones from secondary adrenal insufficiency.
Diagnosis:
magnetic resonance imaging and blood tests.
Treatment:
correction of hormone deficiencies.
surgical decompression may be required.
Many people with pituitary apoplexy develop pituitary hormone deficiencies and require long-term hormone supplementation.
The initial symptoms of pituitary apoplexy are related to the increased pressure in and around the pituitary gland.
The most common symptom, (over 95% of cases) , is a sudden-onset headache located behind the eyes or around the temples.
The sudden headache is often associated with nausea and vomiting.
In 24% of cases bleeding leads to irritation of the meninges, which may cause neck rigidity, photophobia as well as a decreased level of consciousness.
Compression of the optic chiasm leads to a characteristic pattern of vision loss affecting the outer halves of each eye: bilateral hemianopsia it is encountered in 75% of cases.
With pituitary apoplexy visual acuity is reduced in half, and over 60% have a visual field defect.
Adjacent to the pituitary lies the cavernous sinus.
The cavernous sinus contains a number of nerves that control the eye muscles, so 70% of people with pituitary apoplexy experience double vision due to compression of one of the nerves.
In half of these cases of pituitary apoplexy, the third cranial nerve, which controls a number of eye muscles, is affected and leads to diagonal double vision and a dilated pupil.
The fourth and sixth cranial nerves are located in the same compartment and can cause diagonal or horizontal double vision, respectively.
The oculomotor nerve is predominantly affected as it lies closest to the pituitary.
The adrenal glands are typically the first to be affected in pituitary apoplexy.
When the stimulating hormone ACTH is not secreted, the adrenals cease to produce cortisol.
In pituitary apoplexy, the main initial problem is a lack of secretion of adrenocorticotropic hormone (ACTH, corticotropin), which stimulates the secretion of cortisol by the adrenal gland, occurring in 70% of those with pituitary apoplexy.
The sudden lack of cortisol in the body leads to an adrenal crisis, the main cause of adrenal dysfunction and low cortisol levels.
Adrenal crisis: hypotension, particularly on standing, hypoglycemia, and abdominal pain is life-threatening and requires immediate medical attention.
Hyponatremia, an unusually low level of sodium in the blood that may cause confusion and seizures.
Hyponatremia is found in 40% of cases of pituitary apoplexy, and may be caused by low cortisol levels or by inappropriate release of antidiuretic hormone (ADH) from the posterior pituitary.
Addition hormonal deficiencies may develop in the subacute phase of pituitary apoplexy, with 50% have a deficiency in thyroid-stimulating hormone (TSH), leading to hyposecretion of thyroid hormone by the thyroid gland and characteristic symptoms such as fatigue, weight gain, and cold intolerance.
75% of patients with PA develop a deficiency to gonadotropins (LH and FSH), which control the reproductive hormone glands.
The deficiency to gonadotropins (LH and FSH), leads to a disrupted menstrual cycle, infertility, and decreased libido.
Almost all cases of pituitary apoplexy arise from a pituitary adenoma, a benign tumor of the pituitary gland.
In 80% of PA cases the patient has been previously unaware of this process.
Only a very small proportion of pituitary tumors eventually undergoes apoplexy: In incidentally found pituitary tumors, apoplexy occurred in 0.2% annually
The risk is higher in tumors larger than 10 mm and tumors that were growing more rapidly.
In 60–80% of cases it is not precipitated by a particular cause.
Associated with surgery, especially coronary artery bypass graft, where there are significant fluctuations in the blood pressure, disturbances in blood coagulation or medication that inhibits coagulation, radiation therapy to the pituitary, traumatic brain injury, pregnancy and treatment with estrogens, hormonal stimulation tests, treatment of prolactinomas with dopamine agonist drugs, as well as withdrawal of such treatment, has been reported to precipitate apoplexy.
Pituitary apoplexy is as distinct from Sheehan’s syndrome: pituitary undergoes infarction as a result of prolonged very low blood pressure, particularly when caused by bleeding after childbirth.
Some regard Sheehan’s syndrome as a form of pituitary apoplexy.
The pituitary gland is located in a skull recess in the base of the brain, known as the sella turcica.
It is attached to the hypothalamus, a part of the brain, by a stalk that also contains the blood vessels that supply the gland.
Pituitary tumors are five times more likely to bleed than other tumors in the brain.
The pituitary gland normally derives its blood supply from vessels that pass through the hypothalamus.
Tumors develop a blood supply from the nearby inferior hypophyseal artery that generates a higher blood pressure, possibly accounting for the risk of bleeding.
Pituitary tumors may also be more sensitive to fluctuations in blood pressure, and the blood vessels may show structural abnormalities that make them vulnerable to damage.
Infarction alone causes milder symptoms than either hemorrhage or hemorrhagic infarction.
Larger pituitary tumors are more prone to bleeding, and more rapidly growing lesions may also be at a higher risk of apoplexy.
With apoplexy, the pressure inside the sella turcica rises, and surrounding structures such as the optic nerve and the contents of the cavernous sinus are compressed, further impairing the blood supply to the pituitary hormone-producing tissue, leading to tissue death due to insufficient blood supply.
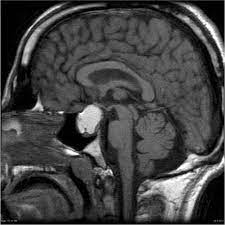
Magnetic resonance imaging (MRI) scan of the pituitary gland is performed if the diagnosis is suspected; this has a sensitivity of over 90% for detecting pituitary apoplexy, demonstrating infarction or hemorrhage/
If MRI is not suitable computed tomography (CT) scan may demonstrate abnormalities in the pituitary gland, although it is less reliable.
Many pituitary tumors (25%) have areas of hemorrhagic infarction on MRI scans, but apoplexy is not said to exist unless it is accompanied by symptoms.
Lmbar puncture examination of the cerebrospinal fluid that envelops the brain and the spinal cord are typically normal, although abnormalities may be detected if blood from the pituitary has entered the subarachnoid space.
Laboratory evaluation for suspected PA includes: complete blood count, renal function tests, electrolytes, liver function tests, routine coagulation testing, and a hormonal panel including IGF-1, growth hormone, prolactin, luteinizing hormone, follicle-stimulating hormone, thyroid-stimulating hormone, thyroid hormone, and either testosterone in men or estradiol in women.
Visual field testing is recommended.
Treatment:
The first priority is stabilization of the circulatory system.
Cortisol deficiency can cause severe hypotension.
Treatment for acute adrenal insufficiency requires the administration of intravenous saline or dextrose solution, followed by the administration of hydrocortisone, intravenously or into a muscle.
If visual acuity is severely reduced, or worsening visual field defects, or the level of consciousness falls consistently, guidelines recommend that surgery is performed.
Most commonly, operations on the pituitary gland are performed through transsphenoidal surgery.
With relatively mild visual field loss or double vision only may be managed conservatively.
Patients who have had pituitary apoplexy require follow-up by an endocrinologist to monitor for long-term consequences.
Mortality is low at 1.6% overall.
80% of people with PA develop hypopituitarism and require some form of hormone replacement therapy.
The most common problem is growth hormone deficiency/ may cause decreased muscle mass and strength, obesity and fatigue.
60–80% require hydrocortisone replacement, 50–60% need thyroid hormone replacement, and 60–80% of men require testosterone supplements.
Finally, 10–25% develop diabetes insipidus, the inability to retain fluid in the kidneys due to a lack of the pituitary antidiuretic hormone.
This may be treated with the drug desmopressin, which can be applied as a nose spray or taken by mouth.