 The jugular venous exam is an important aspect of assessing a patient’s fluid volume status, especially in patients with heart failure, liver failure and kidney failure.
The jugular venous exam is an important aspect of assessing a patient’s fluid volume status, especially in patients with heart failure, liver failure and kidney failure.
Waveforms are often better seen with the head lying directly against the examining table/bed.
Venous waves are bifid, flicking like a snake’s tongue.
It rises when the head of the bed is lowered and sinks when you raise the head of the bed.
Venous waves change with respiration, sinking into the chest with inspiration.
Venous waves are not palpable.
The external jugular vein is observed.
Commonly, the pulsation of the carotid artery is seen and mistaken for that of the JVP.
By pressing on the right upper quadrant the JVP should rise in all individuals, whereas a carotid pulsation should not change.
To measure the jugular venous pressure the highest point of pulsation is recognized, and
Identify JVP at its highest point of pulsation measured from the Angle of Louis, plus 5cm ( to the center of the atrium).
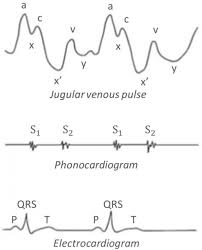
Normal Jugular Venous Waveforms
There are two positive waves ‘a’ and ‘v’, one occurring just before the first heart sound or the carotid impulse, and one just after.
JugularVenousWaveform
“A” wave: atrial contraction, absent in atrial fibrillation.
“C” wave: ventricular contraction (tricuspid bulges). Not seen
“X” descent: atrial relaxation
“V” wave: atrial venous filling, occurs at same of time of ventricular contraction.
“Y” descent: ventricular filling, tricuspid opens
Elevated “a” wave
Resistance to right atrial emptying
May occur at or beyond the tricuspid valve.
Pulmonary Hypertension
Rheumatic tricuspid stenosis
Right atrial mass or thrombus
Cannon “a” waves are large positive venous pulse during “a” wave.
It occurs when an atrium contracts against a closed tricuspid valve during AV dissociation.
Premature atrial/junctional/ventricular beats
Complete atrio-ventricular (AV) block
Ventricular tachycardia
Absent “a” wave
No atrial contraction, common to atrial fibrillation.
Elevated “v” wave
Tricuspid regurgitation is the most common cause.
The ventricle contracts and if the tricuspid valve does not close well, a jet of blood shoots into the right atrium.
Significant Tricuspid regurgitation, will be accompanied by a pulsatile liver, and the murmur of tricuspid regurgitation, a pansystolic murmur that increases on inspiration.
Kussmaul’s sign: neck veins rise in inspiration rather than fall.
It is often a sign of pericardial tamponade or right heart failure, acute right ventricular myocardial infarction.
Friedrich’s sign: exaggerated “x” wave or diastolic collapse of the neck veins from constrictive pericarditis.
The sternal angle (Angle of Louis) is the most popular reference point to use because it remains approximately 5 cm above right atrium regardless of the patient’s position.
The clavicle is approximately 10 cm above the right atrium.