 Utilizes miniaturized transducers placed in catheters during cardiac catheterization.
Utilizes miniaturized transducers placed in catheters during cardiac catheterization.
Intravascular ultrasound (IVUS) is a diagnostic tool used to evaluate the coronary arteries.
It uses a tiny ultrasound probe, mounted on the end of a catheter, which is inserted into a blood vessel and guided to the site of interest.
Once the catheter is in place, the ultrasound probe sends sound waves through the vessel walls, which allow for a detailed, real-time image of the inner lining of the artery to be created.
The images produced by IVUS may help diagnose, treat, and assess certain types of heart disease, including coronary artery disease, stent placement, and assessment of plaque buildup in the arteries.
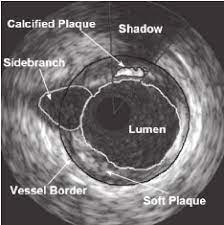
Intravascular imaging provides details of coronary anatomy anatomy that are not seen on angiography.
Coronary artery dimensions and features of plaque and the artery wall can be determined by intravascular imaging.
IVUS allows doctors to see detailed images inside the artery that cannot be picked up by other imaging tools such as angiography, which only shows the external structure of the artery.
It is used to identify and measure the extent of blockages and other issues within the artery, and can be used to assess the appropriateness of stent or other treatments.
Intravascular ultrasound is generally considered safe and is a low-risk procedure.
Measures the degree of stenosis within coronary arteries when coronary angiograms are inconclusive.
Helps guide percutaneous coronary intervention for intermediate coronary stenosis with narrowing of the coronary artery lumen by 40 to 70%.
IVUS is a higher resolution intracoronary imaging method used to select the appropriate stent size and to determine whether the stent is correctly placed and sized after implantation.
IVUS has a role in improving stent implantation that is associated with lower mortality and lower frequency of target vessel revascularization.
IVUS in complicated coronary disease patients who undergo stent implantation versus, angiogram for guidance, is associated with a lower risk of target vessel failure, deaths from cardiac causes, target vessel related myocardial infarction, or clinically driven target vessel revascularization.
Fractional flow reserve and IVUS use is considered to be the best current practice for PCI, although it is estimated that FFR and are used only 18.5% and 13.9% of procedures, respectively.