Intradiscal electrothermal therapy (IDET) is a procedure of applying heat to the annulus in cases of pain due to discogenic conditions that fail to respond to non-operative techniques.
IDET is a minimally invasive surgical procedure for the treatment of discogenic pain.
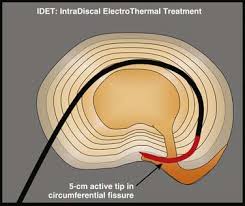
The technique involves applying heat to the annulus fibrosus through a catheter with a temperature-controlled thermal resistive heating coil.
The goal is to damage the nerve fibers, shrink collagen, and stiffen the disc tissue; this might seal any small tears and limit the expression of matrix components.
Mechanical failure of the intervertebral disc is associated with inflammation, dehydration of the nucleus pulposus, decreased disc height, and annular tears.
Discogenic pain may cause chronic lumbago without sciatica; the pain usually increases with exercise, cough, and Valsalva maneuver.
IDET is indicated for disc-related chronic pain.
It is used for a select subgroup of patients with non-radicular low back chronic pain, usually for at least 3 to 6 months, who fail to respond to conservative treatment including nonsteroidal anti-inflammatory drugs (NSAIDs), stretching, light exercise, traction, bracing and/or bed rest.
Failed an intensive non-operative treatment protocol, including non-steroidal anti-inflammatory drugs (NSAIDs), traction, physical therapy and injections.
Patient with persistent low back pain with a normal neurologic exam and without sciatica.
Pain provocation by discography at the affected level and discordant pain at adjacent unaffected levels.
An MRI, which not demonstrate a neural compressive lesion or spinal stenosis.
Annular tears.
Disc protrusions of size less than 3 to 4 mm.
At least 50% remaining disc height.
The gold standard for diagnosing lumbar discogenic pain is a provocative discography.
Before IDET in which a contrast gets injected into the nucleus pulposus of the disc, and concordant pain gets reproduced as intradiscal pressures increases.
Provocative discography may characterize the architecture of the disc, providing both anatomical and functional information about a disc.
Provocative discography may lead to accelerated disc degeneration, including increased incidence of lumbar disc herniations, loss of disk height, and endplate changes.
When patients with chronic lumbar back pain fail to respond to conservative treatment and/or minimal procedures such as injection therapy of the epidural space, radiofrequency, or IDET, surgical treatment should merit consideration.
IDET is contraindicated:
severe disc degeneration with greater than 50% disc height loss
extruded or sequestered herniated disc,
radiculopathy,
spinal stenosis, or spinal instability.
patients with previous lumbar spine surgery or IDET before, within the last six months at the same level
The patient receives conscious sedation plus a local anesthetic as an outpatient procedure.
IDET utilizes a 1.5 or a 5 cm flexible active-tip catheter to be placed in the junction between annulus and nucleus pulposus or in the posterior annulus.
Giving an intravenous dose of prophylactic antibiotics is recommended.
The procedure takes place under biplanar fluoroscopy or C-arm fluoroscopy in which a single needle approach is performed with a stylet needle that ranges in size from 18- to 22- gauge.
A posterolateral extradural approach is preferred to avoid damage to the dural sac.
The standard protocol begins heating the catheter tip at 149 degrees F (65 degrees C) with increments to a final peak of 194 degrees F (90 degrees C).
This temperature is then maintained for approximately 4 minutes.
Antibiotics, either intravenous or injected into the disc, are used to prevent spondylodiscitis.
No intradiscal corticosteroids or other medications should be injected into the disc.
The treatment procedure is repeatable in case there are multiple discogenic pain levels.
Discography and IDET procedures are associated with very low complication rates:
Radiculopathy.
Accelerated disc degeneration
Endplates deformation
Spondylodiscitis
Transthecal puncture route may result in post-procedural headache
Vertebral osteonecrosis
Cauda equina syndrome
The IDET changes disc biomechanics, decreased intradiscal pressure, annular denervation, and sealing annular tears.
There is no consistent evidence regarding the effectiveness of IDET.
Several clinical trials show that patients experience clinical benefit from this procedure, and also physical function scores demonstrated continued significant improvement between the 1- and 2-year observation points.
Pain relief after IDET is not immediate, and may increase during the first couple of days.
Physical therapy is a crucial aspect of recovery.
Categories