 Central retinal artery occlusion (CRAO) is an ophthalmic emergency because irreversible ischemic damage to the retina can occur in as little as 90 minutes.
Central retinal artery occlusion (CRAO) is an ophthalmic emergency because irreversible ischemic damage to the retina can occur in as little as 90 minutes.
It is considered an ocular stroke and the risk of ischemic stroke with large vessel involvement is particularly increased in the first one to four weeks after a diagnosis of a CRAO.
Patients may present with sudden, painless decreased vision in one eye over a matter of seconds.
It may be partial vision loss if one of the smaller distal branches are affected.
Patients may have experienced intermittent transient, painless vision loss.
Risk factors for CRAO include cigarette smoking, hypertension, high body mass index, high serum lipid levels, diabetes, cardiac disease, hypercoagulable conditions such as antiphospholipid antibody syndrome and autoimmune conditions.
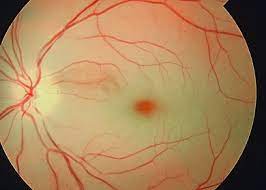
Clinically blanched, non perfused retina, and a cherry red spot due to bright red appearance of the fovea on fundoscopic examination may be apparent.
A boxcar pattern can be seen in the retinal arteries and veins due to segmented blood flow.
No proven therapy exists for retinal artery occlusion.
Digital massage to dislodge the clot to a distal branch and reduce ischemia, anterior chamber paracentesis, and carbogen inhalation have been suggested, all with poor visual outcomes.
Therapy with full dose aspirin and evaluation with carotid imaging and neurological workup, MRI of the brain, echocardiography, Holter monitoring should be performed.
Giant cell arthritis should be ruled out.
Patients should have diet alterations, smoking cessation, and initiation of statin therapy in the case of dyslipidemia.