 Broca’s aphasia is an aphasia in which the output of spontaneous speech is markedly diminished and there is a loss of normal grammatical structure.
Broca’s aphasia is an aphasia in which the output of spontaneous speech is markedly diminished and there is a loss of normal grammatical structure.
Also called expressive aphasia.
Small linking words, conjunctions, such as and, or, and but, and the use of prepositions are lost.
With Broca’s aphasia one may exhibit interjectional speech where there is a long latency, and the words that are expressed are produced as if under pressure.
The ability to repeat phrases is also impaired in patients with Broca aphasia.
The words that are produced are often intelligible and contextually correct.
Comprehension is intact.
Broca aphasia patients are often very upset about their difficulty communicating.
Aphasia describes a disturbance in the ability to use symbols, written or spoken, to communicate information and is categorized into two types: expressive aphasia or receptive aphasia: the two types of aphasia can occur together.
Aphasia is typically considered a cortical sign. Its presence suggests dysfunction of the dominant cerebral cortex.
Aphasia/dysphasia should be distinguished from dysarthria which results from impaired articulation.
Dysarthria, as opposed to aphasia, is a motor dysfunction due to disrupted innervation to the face, tongue, or soft palate that results in slurred speech but intact fluency and comprehension.
The most common cause of Broca aphasia is a stroke involving the dominant inferior frontal lobe or Broca area.
A stroke in Broca area is usually due to thrombus or emboli in the middle cerebral artery or internal carotid artery.
Other causes of Broca aphasia include: traumatic brain injury, tumors, and brain infections.
Aphasia is also a symptom of degenerative dementing illnesses such as Alzheimer disease.
With dementing illness, patients develop gradual progressive language deficits as opposed to a sudden onset of loss of language function that is seen in an ischemic stroke.
There are approximately 170,000 new cases of aphasia related to stroke occur annually.
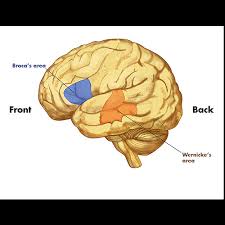
Broca area is a region in the inferior frontal lobe of the dominant hemisphere of the brain made up of Brodmann area 44 and 45.
Language function lateralized to the left hemisphere in 96% to 99% of right-handed people and 60% of left-handed people.
Various pathways connect Broca area to the frontal lobe, basal ganglia, cerebellum, and contralateral hemisphere.
Lesions in the Broca area causes a breakdown between one’s thoughts and one’s language abilities.
Patients often feel that they know what they wish to say but are unable to produce the words.
Broca aphasia patients are unable to translate their mental images and representations to words.
The normal fluency of speech is impaired.
Broca’s area serves a role in ordering sounds into words, and words into sentences, and thus creates relationships between linguistic elements.
Broca aphasia is non-fluent aphasia, with an. output of spontaneous speech that is markedly diminished.
There is a loss of normal grammatical structure, linking words, conjunctions and the use of prepositions are lost.
Patients can exhibit interjectional speech where there is a long latency, and the words that are expressed are produced as if under pressure.
The ability to repeat phrases is also impaired.
Words that are produced are often intelligible and contextually correct, as in pure Broca aphasia, comprehension is intact.
Patients are often very upset about their difficulty communicating.
This angst may be due to the deficit itself or may be due to damage to adjacent frontal lobe structures which control the inhibition of negative emotions.
Broca aphasia can accompany other neurological deficits such as right facial weakness, hemiparesis or hemiplegia, and apraxia.
Examination assesses fluency, the ability to name objects, repeat short phrases, follow simple and complex commands, read, and write.
Nuropsychological testing may be helpful in determining the type and severity of the language deficit.
Neuroimaging (CT, MRI, fMRI, PET or SPECT) may be required to localize and diagnose the cause of aphasia.
Patients should also be screened for depression commonly associated with Broca’s aphasia.
Broca’s aphasia often has a devastating effect on the ability of individuals to carry out their normal activities.
It affects the patient’s ability to communicate and often leads to loss of productivity and vocation and can also lead to social isolation.
Speech and language therapy are the main approaches for patients with aphasia.
It is essential to provide such patients a means to communicate their wants and needs.
Abtreatment option for patients with Broca aphasia is melodic intonation.
Musical ability is often spared in Broca aphasia.
Medical treatment of aphasia is currently under investigation: therapies have included catecholaminergic agents (bromocriptine, levodopa, amantadine, dexamphetamine), piracetam and related compounds, acetylcholine esterase inhibitors, and neurotrophic factors.
Transcranial magnetic stimulation and transcranial direct stimulation trials for aphasia are currently underway.
When the cause of Broca aphasia is a stroke, recovery of language function peaks within two to six months, after which time further progress is minimal.
Differentiatial Zdiagnodis:
Anterior circulation stroke
Cardioembolic stroke
Central pontine myelinolysis
Cerebral venous thrombosis
Dementia in motor neuron disease
Dissection syndrome
Frontal lobe syndrome
Glioblastoma multiforme
Head injury
Recovery after Broca aphasia is often many months or even years, especially if the cause was a stroke.
Most people see mild improvement within the first six months, but full recovery can take years.