 A rare medium and small vessel autoimmune vasculitis leading to necrosis.
A rare medium and small vessel autoimmune vasculitis leading to necrosis.
Referred to as EGPA, eosinophilic granulomatosis with polyangiitis.
EGPA is a mixed allergic and vascular disorder classically associated with a prodrome of allergic rhinitis, chronic sinusitis, an adult onset asthma that can persist for years.
An allergic granulomatous angiitis.
A granulomatous small vessel vasculitis.
Autoimmunity suggested in pathophysiology with the presence of hypergammaglobulinemia, elevated levels of IgE and rheumatoid factor and ANCA.
IL-5 has the central role in EPGA.
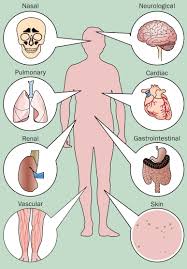
Involves blood vessels of the lung, gastrointestinal system, peripheral nerves, heart, skin, and kidneys.
Non-inherited, non-transmissible process similar to polyarteritis nodosa.
Not associated with an increased risk of malignant transformation.
Associated with eosinophilic and granulomatous infiltration in affected tissues.
Associated with end organ involvement, small vesselvasculitis, and other clinical findings of pulmonary involvement with eosinophil infiltration that causes waxing and waning opacities on radiography, peripheral neuropathy, and signs of cardiac involvement with cardiomyopathy, pericardial effusion, and valvular insufficiency.
Associated with anti neutrophil cytoplasmic antibodies (ANCA).
More than 50% are ANCA negative.
Criteria for diagnosis includes asthma, eosinophilia of more than 10%, mononeuropathy or poly neuropathy, pulmonary infiltrates, paranasal sinus abnormality, and extravascular eosinophilia on biopsy.
A rare premature disorder, characterized by asthma, necrotizing, vasculitis, extravascular granulomas, and blood and tissue eosinophilia.
Anti-neutrophilic cytoplasmic antibodies are found in 30-40% of patients, mainly with a perinuclear immunofluorescence pattern (P-ANCA).
Anti-neutrophilic cytoplasmic antibodies are also ref2242ed to as anti-myeloperoxidase antibodies.
ANCA positive patients have a greater risk of renal and peripheral neuropathy involvement, while ANCA negative patients will more likely have cardiac disease.
Can be difficult to differentiate from Wegener’s granulomatosis.
Wegener’s syndrome associated with c-ANCA, unlike this process which shows elevations of p-ANCA.
Three stages: the first involves sinuses and onset of new allergies or worsening of pre-existing allergies, the second stage involves new onset of asthma, and the third stage involves various other organs and is the most painful and life threatening phase of the disease.
Asthma is a primary feature of this disease, and more than 90% of patients have a history of asthma.
Associated with nerve pain in the extremities.
May be associated with purple skin lesions and nasal and oral mucosal erosions.
Skin involvement present in about two thirds of patients.
Tender subcutaneous nodules on the extensor surface of the arms and legs may be present, and palpable purpura, hemorrhagic lesions ranging from petechiae to ecchymoses, and macular papular erythematous rash may also be seen.
Vesicles may arise when the epidermis separates from ischemic dermis due to superficial blood vessel occlusion.
Skin biopsy reveals a leukocytoclastic vasculitis with the eosinophil infiltration.
May be associated with uvietis.
American College of Rheumatology has 6 criteria for diagnosis: asthma, eosinophilia, of more than 10% in the peripheral blood, paranasal sinusitis, pulmonary infiltrates, and evidence of vasculitis on histologic exam with intravascular eosinophilia ad mononeuritis multiplex or polyneuropathy.
Fulfilling 4 or more criteria of the above have a sensitivity of 85% and a specificity for the diagnosis of Churg-Strauss syndrome of 99.7%.
A similar syndrome occurs as a rare complication of asthma in steroid dependent individuals with leukotriene receptor antagonists with reduction in steroid dose.
Incidence 1-3 cases per 100,000 adults per year.
Major causes of morbidity and mortality are myocarditis and myocardial infarction secondary to coronary arteritis.
Treatment associated with 1-yer survival is 90% and 5 year survival is 62%.
Men are affected more frequently than women by a slight margin.
Age at onset 15-70 years with a mean of 38 years.
The Fve Factors score (FFS) assesses disease severity and guides management.
The five scoring criteria for EGPA, each of which is associated with worse prognosis: older than 65 years, cardiac insufficiency, renal insufficiency, gastrointestinal involvement, and absence of ENT manifestations.
In the above scoring zero is assigned when no factors are present, and one for one factor, two for two or more factors, etc.
Mainstay of treatment is systemic corticosteroid therapy, and most patients achieve remission.
Patients with more severe disease may require alkylating agents such as cyclophosphamide to achieve remission.
Agents utilized include azathioprine , methotrexate, mycophenolate helps to maintain remission.
Mepolizumab and benralizumab target eosinophilic inflammation, that inhibit activation of the differentiation by binding interleukin 5 resulting in remissions and less use of glucocorticoids.