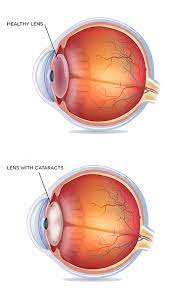
 Involves removal of the cloudy lens from the eye.
Involves removal of the cloudy lens from the eye.
More than half of people age 80 years and older in the US have had cataract surgery.
Cataract surgery and related costs in the United States estimated to be $6.8 billion per year.
Approximately 3 million procedures performed annually.
Cataract surgery improves the quality of life and economic productivity and is associated with lower risk of falling by more than 30%.
Today intraocular lenses are used to replace the removed lens.
Cataract surgery is typically performed through small, self sealing corneal incisions that eliminate the need for sutures.
Cataract surgery uses phacoemulsification where ultrasonic waves delivered through a handheld probe fractures the clouded lens into small fragments through a circular anterior capsulotomy.
These fragments are then aspirated out of the eye while the capsular bags preserved and supports zonules.
A malleable ocular lens is injected into the eye and unfolds in the capsular bag.
The malleable IOL is fixated to the same location as the natural lens, the avascular capsule bag sequesters the prosthetic IOL and minimizes foreign body reaction.
Cataract surgery is safe and has a less than one percent risk of major adverse cardiac events or death and is usually performed an ambulatory setting with topical anesthesia.
Ocular biometry is a test performed to determine the required power of intraocular lens implant receive during cataract surgery.
Lenses have been anterior chamber, posterior chamber and now multi-focal intraocular lenses.
The multifocal intraocular lenses provide full range of vision from distance to near without the need for eyeglasses.
Multifocal intraocular lenses have concentric rings alternating between distance and near vision projecting multiple images onto the retina.
Multifocal intraocular lenses associated with glare at night.
New lenses with adjustable focusing ability are available and they work like the natural lens with flexible hinges at 180 degrees apart from each other, with ciliary muscle contraction causes the implant to move effecting the power of the lens.
A very safe procedure with less than 1% risk of major adverse cardiac events or death.
Individuals who had cataract surgery have a lower risk of developing all cause dementia than those who did not undergo surgery.
Mean duration of procedure is 18 minutes.
Virtually all procedures performed in ambulatory setting with topical anesthesia.
The overall incidence of surgical complications is less than 3% and include: rupture of the posterior capsule with vitreous loss, retinal detachment, iris trauma, and endopthtalmitid, and expulsive hemorrhage.
The most common complication following cataract surgery is transit macular edema causing blurred vision for several weeks to months, which occurs in approximately 0.8% of patients within three months of surgery.
Opacification of the posterior lens capsule behind the IOL can occur several years following surgery, impairing vision, and managed by a central posterior capsulotomy.
Preoperative medical evaluation does not decrease incidence of adverse events and does not improve outcomes of cataract surgery.
Routine medical preoperative testing-EKG, CXR, chemistry analyses, and blood counts-confer no benefit in reducing adverse perioperative medical events during cataract surgery.
Modern cataract surgery is not more medically stressful than other commonly performed procedures on similar populations such as dental surgery, colonoscopy, for which routine history and physical preoperative examinations are not routine performed.
Guidelines recommend against routine preoperative testing for patients undergoing cataract surgery.
There is no evidence to withhold android platelet or anticoagulant therapy before cataract surgery.
After the opacified lens is surgically removed, and interoperative lens must be implanted to replace it focusing power.
The basic monofocal IOL provides a fixed focus and patients will require a new eyeglasses after surgery to optimize distance,, intermediate, and near focus.
Bifocal trifocal and progressive eyeglasses combine multiple corrections into one frame.
Advancing technologies have additional refractory benefits to reduce postoperative dependence on eyeglasses.
Torric IOL‘s correct pre-existing corneal astigmatism by aligning the eye with eye’s astigmatic axis, while presbyopia, correcting IOL‘s reduce dependence on bifocals and trifocals by extending depth of focus or providing multifocality for a wide range of vision.
Some select different IOL designs or refractory targets for each eye.
Light adjustable IOL made from photos sensitive material allows postoperative adjustments of lens power using targeted UV light from a specialized light delivery device to correct residual refractive error.
2 replies on “Cataract surgery”
How much time is there between removal of the cataract and placing the new lens?
Concurrent procedures