 2194
2194
Brown Adipose Tissue (BAT).
White fat stores fat and is an important way of storing our food for the long term.
Brown fat is thought to generate heat to keep a newborn warm, and
Neonates have a lot of brown fat.
Brown adipose tissue is a specialized fat tissue dedicated to thermogenesis, in contrast to white adipose tissue, which serves largely to store calories.
Brown fat cells come from the mesoderm.
Both adipocytes and brown adipocyte may be derived from pericytes.
Pericytes are cells which surround the blood vessels that run through white fat tissue.
Brown adipose tissue is highly specialized for non-shivering thermogenesis, as each cell has a higher number of mitochondria compared to more typical cells.
Brown fat has more capillaries than white fat, supplying tissues with oxygen and nutrients and distribute the produced heat throughout the body.
Several brown adipose tissue depots have been identified.
Brown fat in adults is limited to the neck, shoulders, posterior thorax, and abdomen, and these depots drain directly into the systemic circulation and may lead to more rapid distribution of warmed blood to the rest of the body.
In infants, BAT depots include, but are not limited to: interscapular, supraclavicular, suprarenal, pericardial, para-aortic, peri pancreatic, kidney and trachea.
The brown fat deposits gradually get more white fat-like during adulthood.
In adults, fat depots most often detected in FDG-PET scans are in the supraclavicular, paravertebral, mediastinal, para-aortic and suprarenal areas.
The maximum detectable brown fat mass is approximately 1 kg, and adults 20 to 50 years of age ranges from 50 to 500 g, or 0.1 to 0.5% of the total body mass, and 0.2 to 3% of total adipose tissue mass.
The amount of brown adipose tissue varies according to sex, and has an inverse association with age and BMI
Brown fat cells, two types, have small lipid droplets and numerous iron-rich mitochondria, giving its brown appearance.
It is found in highly vascularized deposits, such as between the shoulder blades, surrounding the kidneys, the neck, and supraclavicular area, and along the spinal cord.
Brown fat is present in some adults.
Initially thought to be present only in newborns.
Throughout adipose tissue beige fat that is induced adrenergically is dispersed.
Beige adipose tissue has varied lipid droplet size and a greater proportion of lipid droplets to mitochondria than white fat, manifesting with a light brown appearance.
In response to cold it activates cycles of energy consumption, wasting calories and releasing heat.
It is brown because it contains mitochondria, and it can generate heat.
Uncoupled, the mitochondria burn fat and glucose, and can generate heat in the cold.
Brown fat consumes glucose when it’s stimulated by cold or by hormones.
Cold is a major death risk for premature neonates.
Numerous factors make infants more susceptible to cold than adults.
Infants have higher ratio of body surface area to body volume.
Infants have a higher proportional surface area of the head.
Allows us to blow off extra calories, that is particularly important for patients with diabetes, and may actually help regulate the blood sugar level.
Plasma levels of branched-chain amino acids (BCAAs) leucine, valine and isoleucine are consistently elevated in patients with insulin resistance and diabetes.
Cold exposure significantly lowers levels of BCAAs in plasma but only in persons who have high levels of BAT activity, suggesting the cold exposure activates catabolism of BCAA in BAT and that BAT can be a primary site of BCAA breakdown..
Located between the scapulae in the back as well as in the supraclavicular area, around the heart, and around the kidneys.
With the development of obesity or diabetes, these brown fat depositions shrink in size and reduce their activity.
People who have brown fat detected on imaging seem to be at reduced risk of cardiac and metabolic conditions, ranging from type 2 diabetes to hypertension and coronary artery disease, with a notably strong effect in people with obesity.
Hormones secreted from the heart and other areas activate brown fat to grow and produce more heat, taking up glucose and fat as well.
The primary source of activation of brown fat is the sympathetic nerve terminals.
Beta-blockers used to treat hypertension may turn brown fat off and increase body weight.
Brown adipose tissue has an important role in the maintenance of body temperature in neonates.
Historically brown adipose tissue has shown rapid involution in early childhood, leaving only vestigial amounts in adults.
Higher likelihood of detection of brown adipose tissue in women and leaner individuals.
Brown adipose tissue, in contrast to white adipose tissue, is involved in energy dissipation rather than storage.
Studies using 18F-fluorodeoxyglucose (18F-FDG) positron emission tomography–computed tomography (PET–CT) prove that BAT is present in adults.
BAT activity notably declining with increasing obesity.
BAT acts to maintain body temperature and as a protector against obesity in times of positive energy balance, burning off excess calories.
BAT and WAT adipocytes differ in morphology.
Mitochondria are present in high numbers in brown adipocytes, compared with white adipocytes.
Mitochondria release chemical energy in the form of heat by uncoupling of oxidative phosphorylation rather than storing it as ATP.
Brown adipocytes have been identified histologically in up to 50% of younger patients, seeded among white adipocytes.
Approximately one brown adipocyte per 100–200 white adipocytes appear within human visceral WAT.
Using 18F-FDG-PET to identify and characterize BAT in adult humans deposits in 7·5% of women and 3·1% of men, located mainly in the cervical, supraclavicular, axillary and paravertebral regions have been identified.
The probability of detection of brown adipose tissue is inversely associated with age, body mass index and outdoor temperature.
Cold-inducible BAT is present in adults, with the largest depots in and around the neck.
In leaner individuals increasing BAT activity offers a degree of protection from obesity.
Estimated that as little as 50 g of BAT would account for 20% of daily energy expenditure.
Association of brown fat tumors and pheochromacytoma has been reported.
Female sex hormones appear to enhance BAT function.
The elevated plasma growth hormone (GH) and IGF-1 levels of active acromegaly are clinically associated with increased lean body mass and reduced fat.
Treatment of athletes with GH increases lean body mass and reduces fat.
GH has been used in the treatment of HIV-associated adipose redistribution syndrome, a disorder characterized by excess truncal WAT.
In a study of 52,000 individuals who had PET/CT scans as part of cancer evaluation were analyzed.
Some adults have brown fat, typically around the neck and shoulders.
Brown adipose tissue contributes to cardiometabolic health.
Brown fat was detected in 10% of participants.
White fat stores energy.
Brown fat is thermogenic, activated by cold conditions, and burns energy.
Higher rates of brown fat are found among women than men (13.8% vs.
4.9%.
Brown fat content diminishes with advancing age.
It is suspected the rate of around 10% of people having brown fat is likely an underestimate: patients instructed to avoid cold exposure, exercise, and caffeine which increase brown adipose tissue visualization on scan.
Among those with brown fat, the rate of type 2 diabetes was 4.6% compared with 9.5% in those with no detected brown fat.
The occurrence of coronary artery disease was significantly lower in those with brown fat, as was cerebrovascular disease, heart failure and hypertension.
Brown fat also was associated with notable improvements in glucose, triglycerides, and HDL-C levels, but no differences were seen in measures of LDL-Cs or total cholesterol.
Leukocyte and platelet counts were significantly decreased in individuals with brown fat,,especially in those with obesity.
The prevalence of type 2 diabetes in those with obesity and brown fat was less than half the rate in those with obesity without brown fat (7.5% vs. 20.3%).
Brown adipose tissue might play a role in mitigating the deleterious effects of obesity.
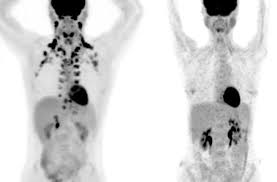
Mirabegron activates brown fat, improves glucose metabolism in healthy women
The drug boosted brown fat activity and improved glucose metabolism in healthy women.
PET images of a woman’s torso show a large increase in brown fat after 28 days.
Too much white fat, a characteristic of obesity, increases the risk of type 2 diabetes, high blood pressure, and other diseases.
Brown fat, breaks down blood sugar and fat molecules to create heat and help maintain body temperature.
Mirabegron is currently approved for a condition called overactive bladder.
The drug binds to a protein on the surface of cells that’s thought to also stimulate brown fat and improve the ability of white fat to break down and release its stored fat into the bloodstream.
After four weeks of treatment, the women’s metabolism at rest was almost 6% higher, although their weight or overall body composition—the ratio of fat to muscle did not change.
Brown fat activity, as measured by PET/CT, also increased during the study, with largest changes in women who had less brown fat activity to begin with.
The women had higher levels of high-density lipoprotein cholesterol and other markers of a reduced risk of heart disease.
Their insulin sensitivity increased by an average of 36%, indicating a reduced risk of diabetes.
Patients experienced increase in resting heart rate, blood pressure, and oxygen consumption while taking the drug.
The observed cardiovascular changes returned to normal two weeks after treatment stopped.
Humans may have less BAT than is required to support their physiologic and metabolic needs.
BAT mass decreases with increased ambient temperatures and aging induces BAT atrophy, raising the possibility that a thermoneutral environment changes artificially lower BAT mass and contribution to energy balance and metabolic health.
The limited BAT present in adults has clinical affects shown by an inverse association between BAT activity and BMI.
Individuals with BAT have healthier blood glucose, triglycerides, and high density lipoprotein levels in persons without BAT.
Patients with BAT have a lower prevalence of cardiometabolic diseases such as type two diabetes dyslipidemia, coronary disease with disease, cerebral vascular disease, congestive heart failure and hypertension.