Adipokines are bioactive signaling molecules secreted by adipose tissue that function as hormones, cytokines, and growth factors to regulate metabolism, inflammation, immunity, and cardiovascular function.
These bioactive proteins secreted by adipose tissue-primarily adipocytes, but also stromal-vascular cells within fat, act locally and systemically, linking metabolic status to immunity, cardiovascular function, and energy homeostasis.
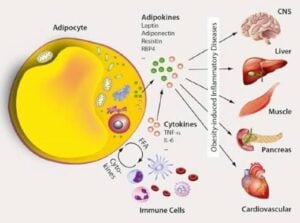
Adipose tissue, once viewed solely as an energy storage depot, is now recognized as the largest endocrine organ in the body, producing numerous adipokines that communicate with the brain, heart, liver, pancreas, skeletal muscle, and vascular system.
Major Adipokines and Their Functions
Adipokines can be broadly categorized based on their predominant effects:
Pro-inflammatory adipokines which are typically elevated in obesity:
Leptin: Regulates appetite and energy expenditure; promotes immune cell activation and cytokine production. Gene: ob gene; receptor OB-R (hypothalamus and periphery) Stimulus for secretion: Increased fat mass, insulin, glucocorticoids Suppresses appetite via hypothalamic arcuate nucleus inhibiting neuropeptide Y.
Resistin: Induces insulin resistance and promotes inflammatory responses.
Chemerin: Contributes to inflammation and metabolic dysfunction.
Retinol-binding protein 4 (RBP4): Associated with insulin resistance.
Plasminogen activator inhibitor-1 (PAI-1): Promotes thrombosis and vascular dysfunction.
IL-6, TNF-α, (monocyte chemoattractant protein) MCP-1: Classical inflammatory cytokines secreted by adipose tissue.
Anti-inflammatory adipokines which are typically reduced in obesity.
Adiponectin: The most abundant adipokine; enhances insulin sensitivity, reduces inflammation, and provides cardiovascular protection.
Omentin: Exhibits anti-inflammatory and insulin-sensitizing properties
FGF21: Promotes metabolic health and cardioprotection
CTRP9: Provides atheroprotective effects
Vaspin: Exerts regulatory anti-inflammatory effects
Adipokines with regulatory or mixed effects:
Visfatin: Exhibits both pro-inflammatory and metabolic regulatory functions
Apelin: Involved in cardiovascular regulation and glucose metabolism
Lipocalin-2: Participates in immune regulation and metabolic processes
In obesity, adipose tissue undergoes remodeling that disrupts the balance between pro- and anti-inflammatory adipokines, creating a chronic low-grade systemic inflammation that contributes to:
Insulin resistance and type 2 diabetes: (Elevated leptin and resistin combined with reduced adiponectin impair insulin signaling)
Cardiovascular disease: Dysregulated adipokines promote endothelial dysfunction, atherosclerosis, hypertension, and thrombosis
Metabolic syndrome: Adipokine imbalance links obesity to the cluster of metabolic abnormalities including dyslipidemia, hyperglycemia, and hypertension
Adipokines modulate immune cell function and contribute to chronic inflammatory diseases including rheumatoid arthritis and osteoarthritis
The leptin-to-adiponectin ratio has emerged as a useful biomarker for assessing metabolic disease risk, with higher ratios indicating greater metabolic dysfunction.
Clinical Implications
Adipokines represent potential therapeutic targets for obesity-related complications.
Adipokine biology reveals that adipose tissue dysfunction—not simply excess adiposity—drives many obesity-related complications through altered endocrine signaling.
AgRP, stimulates POMC Increases energy expenditure Pro-inflammatory; activates macrophages and T cells
In obesity: Leptin resistance develops-high levels, blunted response
Adiponectin
Inversely proportional to fat mass — levels are low in obesity
Actions: Increases insulin sensitivity (activates AMPK in liver and muscle) Anti-inflammatory (inhibits NF-κB) Anti-atherogenic; improves endothelial function Promotes fatty acid oxidation Clinical relevance: Low adiponectin is associated with T2DM, metabolic syndrome, and cardiovascular disease
Resistin Actions: Promotes insulin resistance (by inhibiting insulin signaling Pro-inflammatory; induces TNF-α and IL-6 It is more re clearly linked to inflammation in humans than to insulin resistance
Visfatin (NAMPT) Secreted mainly by visceral adipose tissue Acts as an enzyme (rate-limiting step in NAD⁺ biosynthesis) and as a cytokine Actions: Insulin-mimetic effects; pro-inflammatory Levels are elevated in obesity and T2DM
Chemerin Regulates adipogenesis and adipocyte metabolism Recruits dendritic cells and macrophages (chemoattractant) Elevated in obesity, metabolic syndrome, and inflammatory states Omentin Secreted by visceral stromal-vascular cells (not adipocytes directly) Actions: Enhances insulin signaling, anti-inflammatory, vasodilatory Levels are decreased in obesity — similar pattern to adiponectin
Apelin Acts on APJ receptor Actions: Improves insulin sensitivity, inotropic cardiac effects, vasodilation, anti-obesity effects Levels are paradoxically elevated in obesity but decrease with weight loss
TNF-α and IL-6 also produced by adipose
Technically general cytokines but significantly secreted by adipose macrophages
TNF-α: Promotes insulin resistance by serine phosphorylation of IRS-1 IL-6: Pro-inflammatory; contributes to hepatic insulin resistance; stimulates CRP production in the liver
Clinical Significance
Obesity shifts the adipokine profile toward a pro-inflammatory, insulin-resistant state (↑ leptin, resistin, TNF-α, IL-6; ↓ adiponectin, omentin)
Adipokine dysregulation underlies much of the pathophysiology of metabolic syndrome, T2DM, Non alcoholic liver disease (NAFLD), and cardiovascular disease.