 Bickerstaff’s brainstem encephalitis (BBE) is a rare, autoimmune neurological disorder characterized by a classic triad of symptoms: ophthalmoplegia (eye muscle paralysis), ataxia (loss of coordination), and altered consciousness (ranging from drowsiness to coma).
Bickerstaff’s brainstem encephalitis (BBE) is a rare, autoimmune neurological disorder characterized by a classic triad of symptoms: ophthalmoplegia (eye muscle paralysis), ataxia (loss of coordination), and altered consciousness (ranging from drowsiness to coma).
BBE is a rare autoimmune condition affecting the brainstem.
It’s often misdiagnosed because its symptoms can mimic other neurological disorders.
A clinical spectrum of diseases linked to the anti-GQ1b antibody, which also includes Miller Fisher syndrome (MFS) and Guillain-Barré syndrome (GBS).
Triad of Symptoms: Most patients present with progressive eye movement paralysis, unsteadiness while walking, and impaired consciousness.
Warning signs: • Double vision or drooping eyelids • Unsteady gait or loss of coordination (ataxia) • Drowsiness or reduced consciousness • Weakness or paralysis (in severe cases)
In about 50–90% of cases, symptoms are preceded by a respiratory or gastrointestinal infection (such as Campylobacter jejuni or Haemophilus influenzae) within the previous two weeks.
Symptoms typically develop over days to weeks following an infection or illness.
BBE involves the central nervous system (CNS), specifically the brainstem.
Other Symptoms: Patients may also experience limb weakness, facial paralysis, hyperreflexia (overactive reflexes), or Babinski’s sign.
Diagnosis is primarily clinical, supported by several key investigations:
Serum Antibody Testing: About 66–70% of patients test positive for anti-GQ1b IgG antibodies.
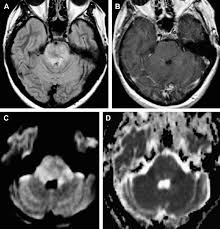
Brain MRI: While often normal in about 70% of cases, an MRI may show lesions in the brainstem, thalamus, or cerebellum on T2-weighted or FLAIR sequences.
* Cerebrospinal Fluid (CSF) Analysis: May reveal albuminocytological dissociation with high protein with normal white cell count or mild pleocytosis with increased cell count.
EEG: Often shows unarousable sleep-like slow-wave activity, reflecting the brainstem’s involvement in consciousness.
Treatment and Prognosis
The mainstay of treatment includes intravenous immunoglobulin (IVIg) and plasmapheresis-plasma exchange, to remove harmful antibodies.
Early recognition leads to faster treatment which can significantly improve outcomes.
High-dose corticosteroids like methylprednisolone are also frequently used.
Despite the severity of the initial symptoms—which can require intensive care and mechanical ventilation—most patients (over 50–70%) make a complete recovery within 6 months.
BBE is typically a monophasic disease, meaning it occurs once and resolves, although rare cases of relapse have been reported.