 Intravascular volume overload is a state of abnormal expansion of the intravascular compartment. It is diagnosed clinically when patients have symptoms, such as symptoms, such as dyspnea, weight gain or edema and signs of excessive volume such as pulmonary crackles, pulmonary and peripheral edema, and jugular venous distention.
Intravascular volume overload is a state of abnormal expansion of the intravascular compartment. It is diagnosed clinically when patients have symptoms, such as symptoms, such as dyspnea, weight gain or edema and signs of excessive volume such as pulmonary crackles, pulmonary and peripheral edema, and jugular venous distention.
Conditions that increase the risk of intravascular volume overload include heart failure, kidney insufficiency, cirrhosis, and excess fluid administration.
Accurate assessment and identification of volume overload, affects clinical decision-making, medication use, and recognition of its presence.
Criterion standards for confirming volume overload or hemodynamic pressure measurements obtained during right heart catheterization, and quantitative blood volume analysis using radio isotope dilution.
Physical examination and point of care, ultrasound findings provide information without delay where is radiologic and laboratory study results take longer to become available.
The accurate assessment of fluid status and its management may prevent complications such as pulmonary edema or poor wound healing associated with peripheral edema.
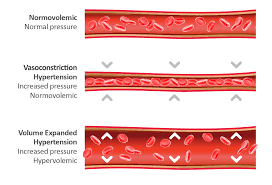
Intravascular volume overload is caused by sodium and water retention, with subsequent plasma volume expansion and increased hydrostatic pressures.
Intravascular volume overload is driven by arterial underfilling with thebody receiving a low effective circulating volume, even if the total blood volume is normal or high.
This process is often associated with heart failure, kidney disease, or cirrhosis, and leads to neurohormonal activation of the renin- angiotensin – aldosterone system, sympathetic nervous system and arginine vasopressin.
Peripheral edema occurs when capillary filtration exceeds the limits of lymphatic drainage with the accumulation of fluid in the interstitial space.
Additional factors that contribute to peripheral edema include increased intravascular hydrostatic pressure due to intravascular volume overload, increased vascular permeability, and plasma oncotic pressure.
Decreased oncotic pressure associated with hypoalbuminemia may be caused by hepatic failure, malnutrition and proteinuria.
Increased intravascular pressure without volume overload may occur in patients with DVT or chronic venous insufficiency.
Peripheral edema is gravity dependent, and usually first develops in the feet and ascends up the legs.
Sacral and scrotal edema are common, particularly in bedbound patients.
Several medications such as calcium channel blockers and gabapentin can cause peripheral edema in the absence of volume overload, primarily through arterial dilation that increases capillary hydrostatic pressure.
Pulmonary crackles occur when small airways pop open during inspiration after being obstructed in expiration due to alveolar fluid accumulation or inflammation.