 Adoptive cell therapy (ACT), or cellular immunotherapy, is a treatment that uses a patient’s own immune cells (or sometimes a donor’s) to find and destroy cancer.
Adoptive cell therapy (ACT), or cellular immunotherapy, is a treatment that uses a patient’s own immune cells (or sometimes a donor’s) to find and destroy cancer.
ACT is a form of cancer immunotherapy that involves isolating, modifying, and expanding immune cells ex vivo, followed by their reinfusion into patients to enhance anti-tumor immune responses.
These cells come from a patient’s blood or tumor, grow them into large numbers in a lab, and then reinfuse them back into the patient.
In many cases, the cells are genetically modified to better recognize and kill specific cancer targets.
Types of Adoptive Cell Therapy
The main types include chimeric antigen receptor (CAR) T-cell therapy, tumor-infiltrating lymphocyte (TIL) therapy, and T-cell receptor-engineered T-cell (TCR-T) therapy.
CAR T-Cell Therapy: T cells are engineered with Chimeric Antigen Receptors (CARs) that allow them to directly bind to proteins on the surface of cancer cells.
This therapy been highly successful for blood cancers like leukemia and lymphoma.
TIL Therapy (Tumor-Infiltrating Lymphocytes): Naturally occurring immune cells that have already entered a patient’s tumor are harvested, expanded, and reinfused.
It is widely used as a standard of care for metastatic melanoma.
TCR-T Therapy (Engineered T-Cell Receptor): T cells are modified with a new T-cell receptor (TCR) that can recognize internal cancer proteins.
Unlike CAR T, this method is “MHC-dependent,” meaning it requires the cancer cells to display those proteins on their surface.
Newer approaches that use Natural Killer (NK) cells or Macrophages instead of T cells are being studied to treat solid tumors and may have lower risks of severe side effects compared to T-cell therapies.
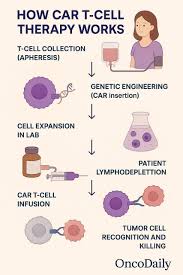
Treatment Process
Cell Collection: A patient’s immune cells are collected through leukapheresis or a tumor biopsy.
The cells are genetically changed (for CAR and TCR-T) and grown into billions of identical “killer” cells over several weeks.
The patient often receives lymphodepleting chemotherapy to clear space in the immune system for the new cells to grow.
Infusion: The concentrated living drug cells is infused back into the patient’s vein to begin hunting the cancer.
Each treatment is tailored to the individual patient’s immune system and cancer type.
Unlike chemotherapy, these cells can persist in the body for long periods, providing ongoing protection against recurrence.
A common side effect is Cytokine Release Syndrome (CRS), a severe inflammatory response that causes high fever and organ stress but is generally manageable with medication.
CAR T-cell therapy involves genetically engineering autologous T cells to express synthetic receptors that recognize tumor cell surface antigens, enabling T cells to attack tumors without requiring major histocompatibility complex (MHC) presentation.
TIL therapy utilizes naturally occurring tumor-reactive lymphocytes isolated from resected tumors, which are expanded ex vivo and reinfused to target tumor-specific antigens.
TCR-T cell therapy involves engineering T cells to express natural T-cell receptors that recognize intracellular tumor proteins presented on MHC molecules.[3][4]
Additional emerging modalities include CAR-natural killer (CAR-NK) cells, CAR-macrophages (CAR-M), cytokine-induced killer (CIK) cells, lymphokine-activated killer (LAK) cells, and dendritic cell (DC) therapies.[5][6][7]
FDA-Approved Indications
6 CAR T-cell products are FDA-approved for hematologic malignancies, targeting CD19 or B-cell maturation antigen (BCMA).
Approved indications include B-cell [acute lymphoblastic leukemia](/rare-disease/acute-lymphoblastic-leukemia), large B-cell lymphoma, follicular lymphoma, mantle cell lymphoma, chronic lymphocytic leukemia, and multiple myeloma.
For solid tumors, lifileucel (a TIL therapy) is FDA-approved for advanced melanoma, and Afamitresgene autoleucel (a TCR-T therapy) is FDA-approved for advanced synovial sarcoma.
No CAR T-cell therapies are currently FDA-approved for solid tumors.
CAR T-cell therapy has demonstrated remarkable efficacy in hematologic malignancies.
In large B-cell lymphoma, CAR T cells improved 4-year overall survival to 54.6% compared with 46.0% for standard chemotherapy followed by stem cell transplant.
In pediatric acute lymphoblastic leukemia, 48% of patients remained alive and relapse-free at 3-year follow-up.
For multiple myeloma, CAR T-cell therapy achieved progression-free survival of 13.3 months compared with 4.4 months with standard therapy in one trial.
Complete or partial remission rates range from 48% to 98% across different CAR T-cell products and malignancies.
The major toxicities associated with CAR T-cell therapy include cytokine release syndrome (CRS), immune effector cell-associated neurotoxicity syndrome (ICANS), prolonged cytopenias, and infections.
Cytokine release syndrome occurs in approximately 40-95% of patients, with grade 3-4 CRS in 2-22%.
CRS typically manifests 2-3 days post-infusion with fever, hypotension, tachycardia, and hypoxia, and may be associated with cardiac, hepatic, and renal dysfunction.
Management includes tocilizumab (an IL-6 receptor blocker) as first-line therapy, followed by glucocorticoids if needed.
Neurologic toxicity (ICANS) affects approximately 15-65% of patients, with grade 3-4 events in 10-28%.
Symptoms typically appear 4-10 days post-infusion and include encephalopathy, delirium, aphasia, tremor, and in severe cases, seizures and cerebral edema.
Glucocorticoids are first-line treatment for ICANS.
Movement disorders have also been reported weeks to months after anti-BCMA CAR T-cell therapies.
Prolonged cytopenias (lasting >28-30 days) affect 22-54% of patients and are believed to be mediated by elevated cytokines.
Severe infections occur in 5-32% of patients, related to immunosuppression and B-cell aplasia following anti-CD19 CAR T-cell therapy.
Long-term B-cell aplasia and hypogammaglobulinemia can occur, requiring immunoglobulin replacement therapy in select patients.
Immune effector cell-associated hemophagocytic lymphohistiocytosis-like syndrome (IEC-HS) is a hyperinflammatory syndrome characterized by cytopenias, hyperferritinemia, coagulopathy, and transaminitis.
Treatment-related mortality is approximately 0-6% in clinical trials of commercially available products.
With earlier use of tocilizumab and glucocorticoids, rates of high-grade CRS have decreased from approximately 9% to 4%.
Adoptive cell therapy challenges include limited efficacy in solid tumors due to tumor heterogeneity, antigen loss, poor trafficking and infiltration, immunosuppressive tumor microenvironment, and T-cell exhaustion.
Strategies to overcome these barriers include multispecific CAR designs, combination with immune checkpoint blockade, targeting the immunosuppressive microenvironment, and development of off-the-shelf allogeneic products.