 Lepidic cancer, officially known as lepidic-predominant adenocarcinoma (LPA), is a specific histologic subtype of non-small cell lung cancer.
Lepidic cancer, officially known as lepidic-predominant adenocarcinoma (LPA), is a specific histologic subtype of non-small cell lung cancer.
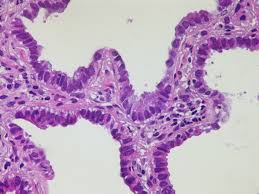
It is characterized by a unique “lepidic” or scaly growth pattern where cancer cells crawl along the surface of intact alveolar walls without initially invading the surrounding lung tissue.
Cells proliferate along existing lung structures.
This pattern is considered non-invasive, unlike other aggressive forms like solid or micropapillary patterns.
It typically presents on CT scans as ground-glassopacities (GGO) or part-solid nodules.
It is more common in women and never-smokers.
Prognosis: Generally, LPA has an excellent prognosis and is slow-growing compared to other lung adenocarcinomas, especially when caught early.
Lepidic growth is used to define three main categories of early lung cancer based on the size and extent of invasion:
Adenocarcinoma in situ (AIS) | Small tumors (3 cm) with pure growth and no invasion. Nearly 100% 5-year survival.
Minimally Invasive Adenocarcinoma (MIA) | Small tumors (3 cm) with lepidic growth and a small invasive area (5 mm).
Approximately 98-100% 5-year survival.
Lepidic Predominant Adenocarcinoma (LPA) | Invasive tumors (>3 cm or > 5 mm invasion where the lepidic pattern is still the dominant feature.
Excellent survival (~90% at 5 years).
It is often found incidentally through CT screening.
Definitive diagnosis requires a biopsy or surgical resection to assess the growth pattern under a microscope.
Treatment: Surgical resection (such as lobectomy or sublobar resection) is the standard treatment.
Because it is often slow-growing, localized surgery is frequently curative.
Molecular markers for mutations like EGFR, KRAS, or ALK rearrangements to guide targeted therapies if the cancer is advanced.
The prognosis can be influenced by invasive components (like micropapillary or solid patterns) mixed within the tumor.