 Sinus tachycardia is a heart rhythm where the sinoatrial (SA) node fires faster than normal, producing a heart rate above 100 beats per minute while maintaining a normal, regular rhythm.
Sinus tachycardia is a heart rhythm where the sinoatrial (SA) node fires faster than normal, producing a heart rate above 100 beats per minute while maintaining a normal, regular rhythm.
The beats originating from the sinoatrial (SA) node, with normal P-wave morphology and axis on electrocardiogram (ECG), reflecting intact conduction through the atria.
The heart rate > 100 bpm originating from the SA node, with normal P waves preceding each QRS complex.
The SA node’s automaticity is governed by the autonomic nervous system, with sympathetic stimulation activating beta-adrenergic receptors to increase cyclic adenosine monophosphate (cAMP), enhance the “funny” current and L-type calcium channels, and accelerate depolarization, while parasympathetic (vagal) stimulation via muscarinic (M2) receptors slows heart rate by increasing potassium efflux and decreasing cAMP.
Sinus tachycardia is classified into three categories: physiologic (appropriate), pathologic (secondary to disease states or pharmacologic agents), and inappropriate sinus tachycardia (IST), a distinct entity in which tachycardia occurs without identifiable physiologic demands.
Pathologic/secondary causes encompass infection and fever, hypovolemia and dehydration, anemia, heart failure and shock, pulmonary embolism, hyperthyroidism, pheochromocytoma, Cushing’s disease, hypoglycemia, and medication or substance effects such as beta-agonists, anticholinergics, caffeine, alcohol, nicotine, amphetamines, cocaine, and beta-blocker withdrawal.
Sinus tachycardia at rest without physiological triggers may represent a spectrum of normal or may indicate serious underlying pathology, and that the classification, consideration of possible etiologies, and decisions of when and how to intervene can be difficult.
Inappropriate Sinus Tachycardia (IST) is a separate diagnosis: a resting rate >100 bpm or exaggerated rate response to minimal exertion with no identifiable cause, likely due to SA node hypersensitivity or autonomic dysregulation.
IST is defined as persistent sinus tachycardia with resting heart rates greater than 100 bpm and average 24-hour heart rates exceeding 90 bpm, accompanied by symptoms such as palpitations, fatigue, lightheadedness, and presyncope, in the absence of identifiable physiologic or pathologic triggers.
The pathogenesis of IST is multifactorial and incompletely understood, with proposed mechanisms including intrinsic sinus node channelopathies affecting the If current, autonomic dysfunction with decreased parasympathetic or increased sympathetic activity, impaired baroreflex control, neurohormonal modulation (involving vasoactive intestinal peptide, histamine, catecholamines, and serotonin), and autoantibody-mediated effects on beta-adrenergic or muscarinic receptors.
IST is a diagnosis of exclusion, requiring elimination of all secondary causes.
The recommended workup includes a comprehensive history and physical examination focusing on potential triggers and underlying causes; a 12-lead ECG to confirm sinus rhythm and exclude other arrhythmias; laboratory studies including complete blood count to assess for anemia, thyroid function tests to exclude thyrotoxicosis, and urine or serum drug screening when indicated; 24-hour Holter or event monitoring to document persistence of tachycardia, correlate symptoms with heart rate, and assess for nocturnal normalization; echocardiography to exclude structural heart disease and cardiomyopathy; and orthostatic vital sign testing with a 10-minute active stand test to distinguish IST from POTS.
Tilt table testing may be indicated when the diagnosis is unclear or symptoms are predominantly orthostatic.
Exercise testing may document an exaggerated chronotropic response but is not routinely validated.
Autonomic testing (heart rate variability, baroreflex sensitivity) is not recommended routinely due to unproven clinical utility.
Psychiatric disorders including panic attacks,anxiety, depression, and somatoform disorders must also be considered, as one report found that 100% of patients with IST had some psychiatric diagnosis.
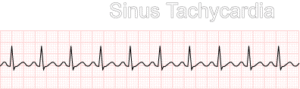
ECG Characteristics of sinus tachycardia: Regular rhythm Rate 100–180 bpm (occasionally higher) Normal P wave morphology (upright in leads I, II) PR interval 0.12–0.20 sec Normal QRS complex
Common Causes Physiological Exercise, anxiety, pain, stress Fever (rate rises ~10 bpm per 1°C) Pregnancy
Pathological: Hypovolemia / dehydration / hemorrhage Anemia Hypoxia / pulmonary embolism Hyperthyroidism Heart failure (compensatory) Sepsis / infection Myocardial infarction
Pharmacological: Stimulants (caffeine, cocaine, amphetamines) Medications: epinephrine, atropine, theophylline, salbutamol Withdrawal (alcohol, beta-blockers) Anticancer treatments, particularly anthracycline compounds, can also trigger sinus tachycardia as part of acute or chronic cardiotoxicity.
Symptoms: palpitations, dizziness, chest discomfort, dyspnea — usually from the underlying cause, not the tachycardia itself.
Workup: 12-lead ECG CBC, metabolic panel, thyroid function Chest X-ray, troponin if cardiac cause suspected Echocardiogram if structural heart disease is a concern
Treatment: Treat the underlying cause — this is the primary intervention.
The management of sinus tachycardia is fundamentally dictated by the underlying etiology.
The AHA guidelines state that for patients with sinus tachycardia, no specific drug treatment is needed; clinicians should focus on identification and treatment of the underlying cause such as fever, dehydration, or pain.
For IST, management is symptom-driven rather than aimed at heart rate normalization, given the generally benign prognosis.
Lifestyle modifications including avoidance of stimulants (caffeine, nicotine), regular exercise, stress reduction, and yoga to increase vagal tone are recommended as initial steps.
Correction of reversible triggers—including fluid resuscitation for hypovolemia, blood transfusion for anemia, infection control for sepsis, withdrawal of offending agents, and management of endocrine disorders—will typically resolve the tachycardia.
Pharmacologic therapy is considered when symptoms are persistent and bothersome.
Beta-blockers may be used symptomatically.
Beta-blockers are the most commonly used agents; metoprolol succinate has been titrated to a target dose of 95 mg daily in studies, but efficacy is limited and side effects including fatigue and hypotension are frequent, with a majority of patients reporting no change or worsening of symptoms.
Non-dihydropyridine calcium channel blockers (verapamil, diltiazem) may be used in patients who cannot tolerate beta-blockers, though their effectiveness is similarly modest.
Ivabradine is an option for inappropriate sinus tachycardia where no cause is found.
Ivabradine, a selective If current inhibitor, has emerged as the most effective and best-tolerated pharmacologic option for IST.
It reduces sinus node automaticity and heart rate without affecting blood pressure or contractility.
The typical dose is 5 to 7.5 mg twice daily, either as monotherapy or in combination with beta-blockers.
Guidelines state that ivabradine is reasonable for ongoing management in patients with symptomatic IST.
In a single-center retrospective analysis, improvement was seen significantly more often with ivabradine than with beta-blockers, though sample sizes were limited.
Recent literature reviews support ivabradine’s role as potential first-line therapy based on its unique mechanism of use-dependent If channel blockade, which provides greater blocking effect at higher tachycardic rates.
Combination therapy with beta-blockers and ivabradine has been shown to resolve symptoms in all patients in small observational studies.
The differential diagnosis of sinus tachycardia is broad.
Physiologic triggers include exercise, emotional stress, pain, anxiety, and pregnancy.
It is essential to distinguish sinus tachycardia from other supraventricular tachycardias, such as atrial tachycardia arising from the crista terminalis and sinus node reentrant tachycardia, which may present with similar rates but have abrupt onset and offset rather than the gradual warm-up and cool-down characteristic of sinus tachycardia.
Postural orthostatic tachycardia syndrome (POTS) must also be differentiated from IST; POTS is characterized by an excessive heart rate increase of ≥30 bpm (≥40 bpm in patients under 20 years) within 10 minutes of standing, without orthostatic hypotension, and with symptoms predominantly related to posture.
For patients with highly symptomatic, drug-refractory IST, procedural options include radiofrequency sinus node modification (SNM), which targets sites of early activation within the SA node.
Acute procedural success rates range from 76% to 100%, but long-term complete resolution of symptoms occurs in only 5.5% of patients, with no long-term benefit in 65.5%.
Complications include symptomatic sinus or junctional bradycardia requiring pacemaker placement, phrenic nerve injury, and superior vena cava syndrome.
Sinus node modification be reserved for patients who are highly symptomatic and cannot be adequately treated by medication.
Novel procedural innovations include intracardiac echocardiography (ICE)-guided anatomical ablation targeting the arcuate ridge, which demonstrated significant heart rate reductions in a small case series with average 24-hour Holter heart rate decreased from 93.2 ± 7.9 bpm to 75 ± 5.6 bpm post-ablation, and sinus node sparing hybrid thoracoscopic ablation, which in a multicenter registry of 100 patients restored normal sinus rhythm in all patients in the hybrid group versus 84% in the RF-SN group, with significantly lower rates of redo procedures (8% vs. 100%).
In catecholamine-induced hypertensive crises, sinus tachycardia is managed with initial alpha-adrenoceptor blockade followed by beta-adrenoceptor blockade, with intravenous verapamil or diltiazem acutely and oral ivabradine for ongoing management.
In athletes, sinus tachycardia is most often a physiological response to exercise.
Sinus tachycardia and premature beats are the most frequent causes of palpitations in athletes, with supraventricular tachycardia, atrial fibrillation, and ventricular tachycardia being much less common.
Persistent sinus tachycardia outside of exercise should prompt evaluation for secondary causes, but the prognosis is excellent in the absence of structural heart disease.
In pregnancy sinus tachycardia as a common benign rhythm disturbance, particularly in the latter half of pregnancy, with basal heart rate increasing by 10 to 20 bpm due to increased sympathetic tone, blood volume expansion, and hormonal changes.
IST has been reported in pregnancy and is associated with a higher frequency of induction at term but without impact on maternal or fetal outcomes.
Approximately 8% of IST cases identify pregnancy as the inciting event.
Post-COVID-19 syndrome has emerged as a significant trigger for IST and POTS.
A prospective study found IST in 20% of post-COVID-19 patients with decreased heart rate variability parameters related to cardiovagal tone.
IST predominantly affects young adults with a female predominance in clinical cohorts, though a population-based study reported no sex differences in prevalence.
In adolescents, a retrospective analysis of 479 patients found 15.4% met criteria for IST (mean 24-hour heart rate ≥95 bpm), with significantly higher risk in those with attention deficit disorder.
POTS affects approximately 500,000 Americans (prevalence ~0.2%), with a strong female predominance (86%) and mean age of 30.2 ± 10.3 years.
Tachycardia-induced cardiomyopathy is a rare but clinically important complication of persistent sinus tachycardia.
The AHA defines it as reversible LV myocardial dysfunction caused by increased ventricular rate, with the degree of dysfunction correlating with duration and rate of the tachyarrhythmia.
Cardiomyopathy secondary to sinus tachycardia is extremely rare, it is not impossible, particularly with sustained rates exceeding 120 to 150 bpm for weeks to months.
Patients homozygous for the ACE gene DD genotype may have greater susceptibility.
The prognosis of physiologic sinus tachycardia is excellent, resolving with correction of the underlying cause.
IST is also generally benign, with rare progression to tachycardia-induced cardiomyopathy, but symptoms can be chronic and debilitating, often lasting five years or more before dissipating.
Management should focus on identifying and treating underlying causes, with no major changes to core algorithms or pharmacologic recommendations.
POTS carries substantial long-term quality-of-life impacts. In a large long-term outcomes survey, 99% of respondents reported ongoing symptoms with a mean symptom duration of nearly 10 years, and the majority experienced moderate to severe limitations in energy, fatigue, and general health.
Over 25% of patients are unable to work, and patients report an average of 3.0 ± 2.8 days lost and 4.7 ± 2.3 unproductive days per week.
Nearly three-quarters of patients experience diagnostic delays, and over half are told their symptoms are psychological in origin.
Depression, anxiety, catastrophizing, and hypervigilance are common comorbidities.
A randomized trial of ivabradine in hyperadrenergic POTS demonstrated statistically significant improvements in both physical functioning and social functioning, with improvements in both physical and mental components achieved with ivabradine monotherapy.
Exercise training remains the most effective non-pharmacologic intervention, counteracting deconditioning and enhancing volume expansion.
However, approximately 50% of patients may experience spontaneous improvement within 1 to 3 years, while for many, symptoms persist and rarely resolve completely
Key controversies include whether ivabradine should be designated first-line therapy for IST, given its superior efficacy and safety profile compared to beta-blockers, though the evidence base remains limited by small sample sizes and the absence of large randomized controlled trials.