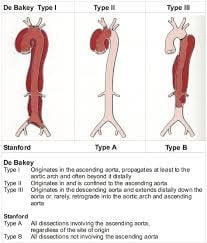
Type B aortic dissection is an aortic dissection that does not involve the ascending aorta, with the intimal tear typically originating at or distal to the left subclavian artery.
In the Stanford classification system—the most widely used framework—type B dissections are distinguished from type A dissections, which involve the ascending aorta, the portion proximal to the innominate artery.
The DeBakey classification further subdivides these as type III dissections, which are limited to the descending and thoracoabdominal aorta.
Most type B dissections begin near the left subclavian artery and extend distally, likely due to high shear forces in this location.
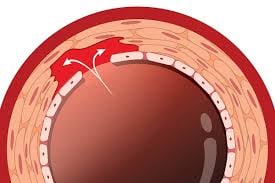
The pathophysiology involves an intimal tear that separates the intima from the media, creating a false lumen where blood flows outside the true aortic lumen.
This can lead to complications if blood flow to aortic side branches becomes compromised.
Type B dissections represent approximately one-third of all aortic dissections, as up to two-thirds of intimal tears originate in the ascending aorta.
Type B dissections are initially managed medically with blood pressure and contractility reduction, whereas type A dissections require emergency surgical intervention.
Surgical or endovascular therapy for type B dissections is reserved for complications such as rupture or end-organ malperfusion.
Acute type B aortic dissection occurs within 14 days of symptom onset, subacute as 15-90 days, and chronic as beyond 90 days.
The temporal classification of type B aortic dissections reflects the evolving pathophysiology and risk profile of the dissection over time.
Complicated type B dissection have persistent or recurrent pain, medication-resistant hypertension, early aortic expansion, malperfusion syndromes that affect renal, visceral, spinal, or lower extremity vasculature, or signs of rupture including hemothorax and increasing periaortic or mediastinal hematoma.
Malperfusion syndrome occurs in approximately 30% of cases and carries early mortality exceeding 30% when mesenteric compromise develops.
Aortic diameter exceeding 40 mm at presentation predicts adverse events, while complete false lumen thrombosis appears protective.
A shorter distance between the primary tear and the left subclavian artery origin predicts aortic growth in uncomplicated cases, whereas a higher number of re-entry tears protects against false lumen expansion.
A “non-A-non-B dissection” describes cases where the dissection involves the aortic arch but spares the ascending aorta, with the entry tear typically between the brachiocephalic and left subclavian arteries.
These account for 3-10% of acute aortic syndromes with treatment options ranging from medical management to open surgical or endovascular approaches.