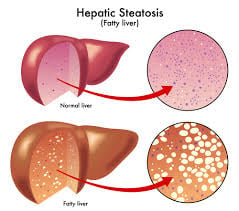
 Hepatic steatosis is the accumulation of excess fat in the liver, typically defined histologically as fat present in more than 5% of hepatocytes or ≥5% of liver weight.
Hepatic steatosis is the accumulation of excess fat in the liver, typically defined histologically as fat present in more than 5% of hepatocytes or ≥5% of liver weight.
Hepatic steatosis/fatty liver is characterized by macrovesicular and/or microvesicular triglyceride droplets within hepatocytes without inflammation or fibrosis.
Steatosis is often graded by percent of hepatocytes involved: grade 0 <5%, grade 1 (mild) 5–33%, grade 2 (moderate) 34–66%, and grade 3 (severe) >66%.
Nonalcoholic causes include metabolic dysfunction–associated fatty liver disease/NAFLD, strongly linked to obesity, insulin resistance, type 2 diabetes, dyslipidemia, metabolic syndrome, rapid weight loss
Non-alcoholic fatty liver disease (NAFLD) – occurs in people who drink little to no alcohol.
Other causes of steatosis include significant alcohol intake, certain drugs (some chemotherapy agents, like corticosteroids, tamoxifen), viral hepatitis, nutritional disorders, and various metabolic or toxic insults.
The key mechanisms for steatosis are: increased influx of fatty acids to the liver, increased de novo lipogenesis, and reduced disposal via β‑oxidation or VLDL export.
Mitochondrial dysfunction, adipokine imbalance, with altered leptin, adiponectin, and pro‑inflammatory cytokines such as TNF‑α contribute to progression from simple steatosis to steatohepatitis and fibrosis.
Simple hepatic steatosis is often asymptomatic and is potentially reversible with risk‑factor modification, particularly weight loss and increased physical activity.
When symptoms do occur, they may include fatigue, general malaise, or mild discomfort in the upper right abdomen.
A subset progress to steatohepatitis (alcoholic or nonalcoholic), then fibrosis, cirrhosis, portal hypertension, and hepatocellular carcinoma; in NAFLD cohorts, 15–30% of NASH patients develop advanced fibrosis, and a proportion of those progress to cirrhosis and HCC.
Evaluation typically includes labs of aminotransferases, metabolic profile, imaging with ultrasound first line, with CT/MRI or quantitative techniques for further characterization, and selectively liver biopsy when the diagnosis is uncertain, to assess the degree of inflammation or fibrosis or staging will alter management.
Management focuses on underlying cause of metabolic fatty liver.
Cornerstone interventions are weight reduction, regular exercise, control of diabetes and dyslipidemia, alcohol avoidance, and review of potentially steatogenic medications.
5-10% of body weight can significantly improve the condition.
Currently, no medications are specifically approved for NAFLD, though some are being studied.
Pharmacologic therapy is generally reserved for high‑risk NASH in guideline‑directed settings.
Alcoholic fatty liver disease (AFLD) – results from excessive alcohol consumption and is the earliest stage of alcohol-related liver disease.
For alcoholic steatosis, chronic heavy drinking is the primary cause.
Most people with hepatic steatosis have no symptoms, especially in early stages.
Simple steatosis with fat accumulation alone, is generally benign, but it can progress to steatohepatitis (fat plus inflammation), which may lead to fibrosis, cirrhosis, and rarely liver cancer if left untreated.