 Functional magnetic resonance imaging or functional MRI (fMRI) measures brain activity by detecting changes associated with blood flow.
Functional magnetic resonance imaging or functional MRI (fMRI) measures brain activity by detecting changes associated with blood flow.
Cerebral blood flow and neuronal activation are coupled. When an area of the brain is in use, blood flow to that region also increases.
The primary form of fMRI uses the blood-oxygen-level dependent (BOLD) contrast.
This specialized brain and body scan used to map neural activity in the brain or spinal cord by imaging the change in blood flow’s hemodynamic response related to energy use by brain cells.
fMRI does not involve the use of injections, surgery, the ingestion of substances, or exposure to ionizing radiation.
This measure is frequently corrupted by noise.
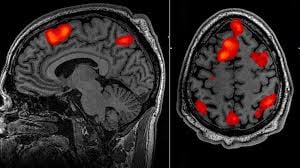
Brain activation can be graphically represented by color-coding the strength of activation across the brain or the specific region studied, localizing activity to within millimeters.
Diffusion MRI is similar to BOLD fMRI but provides contrast based on the magnitude of diffusion of water molecules in the brain.
fMRI can complement other measures of brain physiology such as electroencephalography (EEG), and near-infrared spectroscopy (NIRS).
The fMRI concept builds on the earlier MRI scanning technology and uses a strong, uniform, static magnetic field to align the spins of nuclei in the brain region being studied.
Another magnetic field, with a gradient strength rather than a uniform one, is then applied to spatially distinguish different nuclei, and a radiofrequency (RF) pulse is applied to flip the nuclear spins.
After the RF pulse, the nuclei return to their original equilibrium spin populations, and the energy they emit is measured with a coil.
The use of the gradient field allows the positions of the nuclei to be determined. MRI thus provides a static structural view of brain matter.
fMRI extends MRI to capture functional changes in the brain caused by neuronal activity.
Differences in magnetic properties between arterial (oxygen-rich) and venous (oxygen-poor) blood provided this link.
Changes in blood flow and blood oxygenation in the brain (brain hemodynamics) are closely linked to neural activity.
When neurons become active, local blood flow to those brain regions increases, and oxygen-rich blood displaces oxygen-depleted blood around 2 seconds later.
This rises to a peak over 4–6 seconds, before falling back to the original level, and typically undershooting slightly.
Oxygen is carried by the hemoglobin molecule in red blood cells.
Deoxygenated hemoglobin (dHb) is more magnetic than oxygenated hemoglobin (Hb), which is virtually resistant to magnetism.
This difference leads to an improved MR signal since the diamagnetic blood interferes with the magnetic MR signal less.
This improvement can be mapped to show which neurons are active at a time.
The brain does not store a lot of glucose, the primary source of energy.
When neurons become active, getting them back to their original state of polarization requires actively pumping ions across the neuronal cell membranes, in both directions.
The energy for those ion pumps is mainly produced from glucose.
More blood flows in to transport more glucose, also bringing in more oxygen in the form of oxygenated hemoglobin molecules in red blood cells, and occurs from both a higher rate of blood flow and an expansion of blood vessels.
The blood-flow change is localized to within 2 or 3 mm of where the neural activity is.
Usually the brought-in oxygen is more than the oxygen consumed in burning glucose and this causes a net decrease in deoxygenated hemoglobin (dHb) in that brain area’s blood vessels.
This changes the magnetic property of the blood, making it interfere less with the magnetization and its eventual decay induced by the MRI process.
The cerebral blood flow (CBF) corresponds to the consumed glucose differently in different brain regions.
The initial inflow consumption of glucose in regions such as the amygdala, basal ganglia, thalamus and cingulate cortex is high as these sites are recruited for fast responses.
In regions that are more deliberative, such as the lateral frontal and lateral parietal lobes, the incoming flow is less than consumption.
Hemoglobin differs in how it responds to magnetic fields, depending on whether it has a bound oxygen molecule.
The deoxygenated molecule is more attracted to magnetic fields.
T2 decay, also known as transverse relaxation, is a concept from nuclear magnetic resonance (NMR) and magnetic resonance imaging (MRI).
It describes the process by which the transverse magnetization of a spin system decreases over time due to interactions among spinning nuclei.
When a sample is placed in a magnetic field and subjected to a radiofrequency pulse, the nuclear spins are excited and align perpendicular to the magnetic field.
After the pulse is turned off, the nuclei begin to relax back to their original alignment, and the transverse magnetization decays.
The time constant associated with this decay is referred to as T2, and it is a characteristic property of the material being studied, influenced by factors such as molecular motion, temperature, and the local environment of the nuclei.
A shorter T2 value indicates faster decay and generally results in lower signal intensity in MRI images, whereas a longer T2 value means slower decay and higher signal intensity.
T2 decay is essential for analyzing tissue properties and diagnosing various medical conditions in imaging studies.
Thus MR pulse sequences sensitive to T2* show more MR signal where blood is highly oxygenated and less where it is not.
This effect increases with the square of the strength of the magnetic field.
The fMRI signal hence needs both a strong magnetic field (1.5 T or higher) and a pulse sequence such as EPI, which is sensitive to T2* contrast.
The physiological blood-flow response largely decides the sensitivity, and accuracy we can measure when neurons are active, in BOLD fMRI.
The basic time resolution parameter is designated TR.
The TR dictates how often a particular brain slice is excited and allowed to lose its magnetization.
TRs could vary from the very short (500 ms) to the very long (3 s).
For fMRI specifically, the hemodynamic response lasts over 10 seconds, rising peaking at 4 to 6 seconds, and then falling.
The changes in the blood-flow system, the vascular system, integrate responses to neuronal activity over time.
The change in the MR signal from neuronal activity is called the hemodynamic response.
The hemodynamic response lags the neuronal events triggering it by a couple of seconds, since it takes a while for the vascular system to respond to the brain’s need for glucose.
The hemodynamic response From this point it typically rises to a peak at about 5 seconds after the stimulus.
After activity stops, the BOLD signal falls below the original level, the baseline, in a phenomenon called the undershoot, and over time the signal recovers to the baseline.
The neural system provides feedback to the vascular system of its need for more glucose by releasing glutamate as part of neuron firing.
This glutamate affects nearby supporting cells, astrocytes, causing a change in calcium ion concentration.and releases nitric oxide at the contact point of astrocytes and intermediate-sized blood vessels, the arterioles.
Nitric oxide is a vasodilator causing arterioles to expand and draw in more blood.
The vascular arterial system supplying fresh blood branches into smaller and smaller vessels as it enters the brain surface and within-brain regions, culminating in a connected capillary bed within the brain.
The signal from the large veins needs to be suppressed, since it does not correspond to the area where the neural activity is.
fMRI can examine a spatial range from millimeters to centimeters, and can hence identify Brodmann areas, subcortical nuclei such as the caudate, putamen and thalamus, and hippocampal subfields such as the combined dentate gyrus and subiculum.
Temporal resolution is the smallest time period of neural activity reliably separated out by fMRI.
The time resolution needed depends on brain processing time for various events.
What the eye sees is registered on the photoreceptors of the retina within a millisecond or so, and its signals get to the primary visual cortex via the thalamus in tens of milliseconds.
Neuronal activity related to the act of seeing lasts for more than 100 ms.
A fast reaction, such as swerving to avoid a car crash, takes around 200 ms.
By about half a second, awareness and reflection of the incident sets in.
Remembering a similar event may take a few seconds, and emotional or physiological changes such as fear arousal may last minutes or hours.
Learned changes, such as recognizing faces or scenes, may last days, months, or years.
Most fMRI experiments study brain processes lasting a few seconds, with the study conducted over some tens of minutes.
When a person performs two tasks simultaneously or in overlapping fashion, the BOLD response is expected to add linearly.
The refractory period does not change with age, nor do the amplitudes of hemodynamic responses, but the period differs across brain regions.
In both the primary motor cortex and the visual cortex, the hemodynamic responses amplitude scales linearly with duration of a stimulus or response.
BOLD contrast reflects mainly the inputs to a neuron and the neuron’s integrative processing within its body, and less the output firing of neurons.
Both inhibitory and excitatory input to a neuron from other neurons sum and contribute to the BOLD signal.
Within a neuron these two inputs might cancel out.
The BOLD response can also be affected by disease, sedation, anxiety, medications that dilate blood vessels.
The amplitude of the BOLD signal does not necessarily reflect behavioral performance.
A complex cognitive task may initially trigger high-amplitude signals associated with good performance, but as the subject gets better at it, the amplitude may decrease with performance staying the same.
fMRI helps assess how risky brain surgery or similar invasive treatment is for a patient and to learn how a normal, diseased or injured brain is functioning.
fMRI maps the brain with fMRI to identify regions linked to critical functions such as speaking, moving, sensing, or planning.
This is useful to plan for surgery and radiation therapy of the brain.
Patients with brain pathologies are more difficult to scan with fMRI than are young healthy volunteers.
Tumors and lesions can change the blood flow in ways not related to neural activity, masking the neural hemodynamic response.
Drugs such as antihistamines and even caffeine can affect hemodynamic response.
fMRI has been used clinically to map functional areas, to check left-right hemispherical asymmetry in language and memory regions, check the neural correlates of a seizure, to study how the brain recovers partially from a stroke, and test how well a drug or behavioral therapy works.
The mapping of functional areas by fMRI and understanding lateralization of language and memory help surgeons avoid removing critical brain regions when they have to operate and remove brain tissue.
Recovered depressed patients have shown altered fMRI activity in the cerebellum, and this may indicate a tendency to relapse.
Pharmacological fMRI, assaying brain activity after drugs are administered, can be used to check how much a drug penetrates the blood–brain barrier and dose vs effect information of the medication.
Noise is unwanted changes to the MR signal from elements not of interest to the study.
The five main sources of noise in fMRI are thermal noise, system noise, physiological noise, random neural activity and differences in both mental strategies and behavior across people and across tasks within a person.
Physiological noise is from head and brain movement in the scanner from breathing, heart beats, or the subject fidgeting, tensing, or making physical responses such as button presses.
Head movements cause the voxel-to-neurons mapping to change while scanning is in progress.
Another source of physiological noise is the change in the rate of blood flow, blood volume, and use of oxygen over time.
This last component contributes to two-thirds of physiological noise, which, in turn, is the main contributor to total noise.
In general, fMRI studies acquire both many functional images with fMRI and a structural image with MRI.
It is common to combine fMRI signal acquisition with tracking of participants’ responses and reaction times, such as heart rate, breathing, skin conductance (rate of sweating), and eye movements.
FMRI can also be combined with other brain-imaging techniques such as transcranial stimulation, direct cortical stimulation and, especially, EEG.
The fMRI procedure can also be combined with near-infrared spectroscopy (NIRS) to have supplementary information about both oxyhemoglobin and deoxyhemoglobin.
The fMRI technique can noninvasively record brain signals without risks of ionizing radiation inherent in other scanning methods, such as CT or PET scans.
It can also record signal from all regions of the brain, unlike EEG/MEG, which are biased toward the cortical surface.
fMRI temporal resolution is poorer than that of EEG since the hemodynamic response takes tens of seconds to climb to its peak.
Combining EEG with fMRI is powerful because the two have complementary strengths—EEG has high temporal resolution, and fMRI high spatial resolution.
The strong static magnetic field can cause damage by pulling in nearby heavy metal objects converting them to projectiles.
BOLD contrast depends on blood flow, which is both sluggish in response to stimulus and subject to noisy influences.
The initial burning of glucose raises the temperature, and the subsequent inflow of fresh, cold blood lowers it, and these changes alter the magnetic properties of tissue.
External agents such as thulium compounds are used to enhance the effect.
First, most evidence supporting fMRIs accuracy was done in a lab under controlled circumstances with solid facts.
fMRI has poor reliability when it comes to individual cases, but good reliability when it comes to general human thought patterns.