 Oxalate nephropathy is a kidney condition caused by the deposition of calcium oxalate crystals in the renal tubules and interstitium, leading to acute or chronic kidney injury.
Oxalate nephropathy is a kidney condition caused by the deposition of calcium oxalate crystals in the renal tubules and interstitium, leading to acute or chronic kidney injury.
The process occurs when oxalate levels in the urine exceed the solubility threshold for calcium oxalate, causing crystal precipitation.
These oxalate crystals can obstruct tubules, trigger inflammatory responses, and lead to tubular necrosis and interstitial fibrosis.
Causes:
Primary hyperoxaluria results from rare genetic enzyme defects affecting oxalate metabolism, leading to excessive endogenous oxalate production.
Secondary hyperoxaluria is more common and can result from: Dietary excess of foods high in oxalate like spinach, rhubarb, nuts.
Enteric hyperoxaluria frommalabsorption disorders, bariatric surgery, inflammatory bowel diseases.
Vitamin C megadoses which are metabolized to oxalate.
Ethylene glycol poisoning
Certain medications
Presentation:
Acute oxalate nephropathy presents with rapid decline in kidney function, often with oliguria or anuria.
Patients may experience flank pain, nausea, and vomiting.
Chronic forms develop more insidiously with progressive kidney dysfunction, recurrent kidney stones, and potential end-stage renal disease.
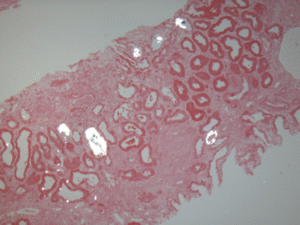
Diagnosis involves identifying oxalate crystals in urine sediment, elevated urinary oxalate excretion, and kidney biopsy showing characteristic birefringent crystals under polarized light.
Imaging may reveal nephrocalcinosis or stones.
Treatment
Management focuses on reducing oxalate load through dietary restriction, adequate hydration, and treating underlying causes.
There is no effective treatment for oxalate nephropathy, and in the short term volume repletion can reduce kidney injury by decreasing the concentration of calcium oxide in the tubules.
Calcium supplementation can bind dietary oxalate.
In severe cases, dialysis may be necessary.
For primary hyperoxaluria, liver transplantation may be required to correct the enzyme deficiency.
Long-term therapy named that preventing further deposition of crystals by means of low fat and low oxalate diet, increased fluid intake, calcium supplementation to increase the binding of enteric oxalate, and treatment of underlying conditions conferring a predisposition to hyperoxaluria.
Early recognition and intervention are crucial to prevent irreversible kidney damage.