”
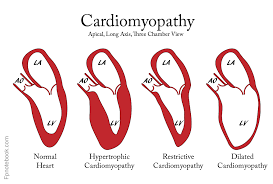
Restrictive cardiomyopathy (RCM) is a form of cardiomyopathy in which the walls of the heart are rigid, but not thickened.
The heart is restricted from stretching and filling with blood properly.
RCM is the least common of the three original subtypes of cardiomyopathy: hypertrophic, dilated, and restrictive.
Untreated hearts with RCM often develop the following characteristics:
Biatrial enlargement Thickened LV walls, with normal chamber size
Thickened RV free wall with normal chamber size
Elevated right atrial pressure (>12mmHg)
Moderate pulmonary hypertension
Normal systolic function
Poor diastolic function, typically Grade III – IV Diastolic heart failure.
Patients will experience decreased exercise tolerance, fatigue, jugular venous distention, peripheral edema, and ascites.
Arrhythmias and conduction blocks are common with RCM.
RCM can be caused by genetic or non-genetic factors, and can be divided into primary and secondary causes.
The common organization is into Infiltrative, storage diseases, non-infiltrative, and endomyocardial etiologies.
Genetic causes DES (desmin) CRYAB (alpha B Crystallin, HSPB5) FLNC (filamin C)
Infiltrative causes Amyloidosis Sarcoidosis Primary hyperoxaluria Storage diseases Fabry disease Gaucher disease Hereditary hemochromatosis Glycogen storage disease Mucopolysaccharidosis type I (Hurler syndrome) Mucopolysaccharidosis type II (Hunter syndrome) Niemann-Pick disease Non-infiltrative Idiopathic Diabetic cardiomyopathy Scleroderma Myofibrillar myopathies Pseudoxanthoma elasticum Sarcomeric protein disorders Werner’s syndrome Endomyocardial Carcinoid heart disease Endomyocardial fibrosis Idiopathic Hypereosinophilic syndrome Chronic eosinophilic leukemia Drugs (anthracyclines, serotonin, methysergide, ergotamine, mercurial agents, busulfan) Endocardial fibroelastosis Consequence of cancer or cancer therapy Metastatic cancer Radiation
The most common cause of restrictive cardiomyopathy is amyloidosis.
Cardiac rhythm and contractility may be normal, but the stiff walls of the heart chambers keep them from adequately filling, reducing preload and end-diastolic volume.
lood flow is reduced, and blood volume that would normally enter the heart is backed up in the circulatory system.
In time, restrictive cardiomyopathy patients develop diastolic dysfunction and eventually heart failure.
Diagnosis is typically made by echocardiography.
Echocardiography demonstrates normal systolic function, diastolic dysfunction, and a restrictive filling pattern.
2-dimensional and Doppler studies are necessary to distinguish RCM from constrictive pericarditis.
Doppler studies present poorly maintained ventricular filling on the E-wave and little to no late ventricular filling on the A-wave leading to the dip and plateau pattern of the early diastolic pressure marks seen on the ECG.
Troponin T, B-type natriuretic peptide (BNP), and pro-DNP biomarkers can also help diagnose RCM.
Cardiac MRI and transvenous endomyocardial biopsy may also be helpful in some cases.
Reduced QRS voltage on EKG may be an indicator of amyloidosis-induced restrictive cardiomyopathy.
Treatment of restrictive cardiomyopathy should focus on management of causative conditions and slowing the progression of cardiomyopathy.
Salt-restriction, diuretics, angiotensin-converting enzyme inhibitors, and anticoagulation are indicated for managing restrictive cardiomyopathy.
Because of reduced blood flow through the heart, there is an elevation in filling pressures.
The excessive use of diuretics may lead to inadequate blood perfusion in body tissues and, consequently, tissue hypoperfusion due to a reduction in overall blood volume.
Calcium channel blockers are generally contraindicated due to their negative inotropic effect, particularly in cardiomyopathy caused by amyloidosis.
Digoxin, calcium channel blocking drugs and beta-adrenergic blocking agents provide little benefit, except in the subgroup of restrictive cardiomyopathy with atrial fibrillation.
Vasodilators are also typically ineffective because systolic function is usually preserved in cases of RCM.
Heart failure resulting from restrictive cardiomyopathy will usually eventually treated by cardiac transplantation or left ventricular assist device.
Endomyocardial fibrosis is generally limited to the tropics and sub-saharan Africa.
The highest incidence of death caused by cardiac sarcoidosis is found in Japan.