 Right bundle branch block (RBBB) is a condition that affects the electrical conduction system of the heart.
Right bundle branch block (RBBB) is a condition that affects the electrical conduction system of the heart.
The right bundle branch (RBB) is a vital component of the heart’s electrical conduction system.
A right bundle branch block (RBBB) is a heart block in the right bundle branch of the electrical conduction system.
In a normal heart, the electrical impulses travel through the right bundle branch to coordinate the contraction of the right ventricle.
The right bundle branch (RBB) consists of specialized nerve fibers (Purkinje fibers) that carry electrical signals from the Atrioventricular (AV) node to the right ventricle, triggering it to contract and pump blood to the lungs.
The right bundle branch (RBB) branches off the Bundle of His at the top of the interventricular septum and courses down toward the apex of the heart before ramifying into the right ventricular walls.
The RBB ensures the right ventricle contracts almost simultaneously with the left ventricle to maintain efficient blood flow.
In RBBB, there is a delay or blockage in the conduction of these impulses.
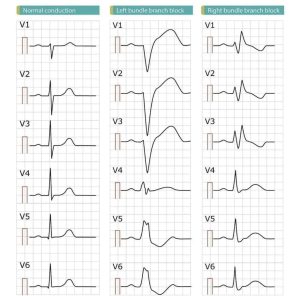
ECG characteristics of a typical RBBB showing wide QRS complexes with a terminal R wave in lead V1 and a prolonged S wave in lead V6.
During a right bundle branch block, the right ventricle is not directly activated by impulses travelling through the right bundle branch.
The left ventricle, however, is still normally activated by the left bundle branch.
It primarily receives blood from the septal branches of the Left Anterior Descending (LAD) coronary artery.
RBBB is usually an incidental finding and may not cause any symptoms or health problems.
It can occur in individuals with normal hearts or can be associated with certain underlying conditions or factors such as heart disease, lung diseases, high blood pressure, and congenital heart defects.
If RBBB is present, it is important to address the underlying cause if one exists.
In most cases, treatment is not required for isolated RBBB.
However, if it is associated with an underlying condition, managing that condition may be necessary.
These impulses are then able to travel through the myocardium of the left ventricle to the right ventricle and depolarize the right ventricle this way.
As conduction through the myocardium is slower than conduction through the Bundle of His-Purkinje fibres, the QRS complex is seen to be widened.
The QRS complex often shows an extra deflection that reflects the rapid depolarisation of the left ventricle followed by the slower depolarisation of the right ventricle.
Incomplete right bundle branch block (IRBBB) is an conduction abnormality in the right bundle branch block.
A complete RBBB has a QRS duration of 120 ms or more, an incomplete block has a wave duration between 110 and 120 ms.
Right Bundle Branch Block (RBBB):
A block occurs when the electrical impulse is delayed or interrupted along this pathway.
This causes the right ventricle to contract slightly later than the left because the signal must travel through the heart muscle from the left side instead of using the fast electrical pathway.
Symptoms: RBBB usually causes no symptoms and is often found incidentally during a routine ECG.
In rare cases, it can lead to fainting or palpitations.
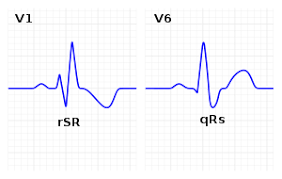
Diagnosis: RBBB is identified on an ECG by a widened QRS complex (≥120 ms for complete block) and a characteristic rabbit ear (RSR’) pattern in lead V1.
Associated;
Normal aging and structural changes.
Heart conditions: Heart attack, cardiomyopathy, or myocarditis.
Lung conditions: Pulmonary embolism, COPD, or pulmonary hypertension.
Procedures: Temporary blocks can occur during right heart catheterization.
Healthy Individuals: If no underlying heart disease is present, RBBB is generally considered benign and typically requires no treatment.
Known Heart Disease: In patients with existing heart failure or a history of heart attacks, RBBB may indicate a higher risk of complications and requires closer monitoring.
Pacemakers: A pacemaker is rarely needed for RBBB alone; it is usually only required if the block is accompanied by other significant conduction problems.
It has a relatively high prevalence,with a mean age of 19 year old military recruits found to have a prevalence of 13.5%.
It affects patients of all ages, more commonly inmales and athletes.
It is not always a benign finding.
It is defined by the following finding in adults:
QRS wave duration between 110 and 120 ms.
rsr, rsR, or rSR in leads V1 or V2.
S wave of longer duration than R wave or greater than 40 ms in leads I and V6.
Normal R wave peak time in both V5 and V6, but greater than 50 ms in V1.
The first three criteria are needed for diagnosis.
The fourth is needed when a pure dominant R waver is present on V1.
Common causes include: normal variation, changes in bundle branch structure – such as mechanical stretching, chest trauma, right ventricular hypertrophy or strain, congenital heart disease such as atrial septal defect, and ischemic heart disease.
A right bundle branch block may also result from Brugada syndrome, pulmonary embolism, rheumatic heart disease, myocarditis, cardiomyopathy, or hypertension.
Causes for incomplete right bundle branch block are exercise-induced right ventricular remodeling, increased RV free wall thickness, especially in athletes due to prolonged endurance exercise.
The heart rhythm originates above the ventricles in the sinoatrial node, atria or atrioventricular node to activate the conduction system at the correct point.
The QRS duration must be more than 100 ms in incomplete block) or more than 120 ms in complete block.
There should be a terminal R wave in lead V1 denoted by R, rR’, rsR’, rSR’, or qR.
There must be a prolonged S wave in leads I and V6, sometimes referred to as a “slurred” S wave.
The T wave should be deflected opposite the terminal deflection of the QRS complex, an appropriate T wave discordance with bundle branch block.
A concordant T wave may suggest ischemia or myocardial infarction.
The underlying condition may be treated by medications to control hypertension or diabetes, if they are the primary underlying cause.
If coronary arteries are blocked, an invasive coronary angioplasty may relieve the impending RBBB.
Prevalence of RBBB increases with age due to changes in the heart’s conduction system.
It’s estimated up to 11.3% of the population by the age of 80 have RBBB.
Does not affect the initial 40-60 ms of the QRS vector and Q waves diagnostic of an acute myocardial infarction are inscribed in RBBB.