 Known as near sightedness.
Known as near sightedness.
Inability to obtain proper focus of distant objects without corrective eyewear or refractive surgery.
Associated with blurry vision that is correct with glasses, contact lenses or refractory surgery.
Among the most common problems in ophthalmologic practice.
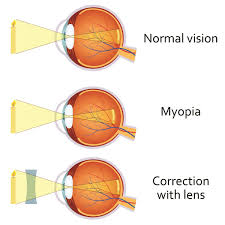
In myopia eye growth continues beyond the normal length, so light rays become focused in front of the retina unless the light is reflected with glasses or contacts lenses or refractory surgery to refocus the light to the retina.
Typically myopia onset occurs between eight and 13 years and stabilizes in late adolescence to early adulthood.
If disproportionate eye growth advances to more than -6 dpt, it can become pathologic.
More than 30% of US population affected.
Lifetime prevalence reported to be 80%-90% in Asia, and other parts of the world the prevalence is almost 50% with more than 40% in the US.
Myopia is experiencing an epidemic rise across the world.
It is increasing in prevalence, and is occurring faster than can be attributed to genetics alone: environmental factors seem to underlie the rapid increase.
The increased incidence of myopia is related to less time spent outdoors and increased near work time.
Its increase is most dramatic among younger people in East and South Asia where the prevalence has reached almost 100 percent in some demographics.
One of the leading causes of vision impairment and blindness in the world.
Increasing degrees of myopia, put patients at greater risk of sight, threatening complications, such as myopic maculopathy, retinal detachment, glaucoma, and cataracts:all of which can lead to severe visual impairment to a blindness.
For every 1.00 D of myopia, the chance of having myopic maculopathy increases by 67%.
The onset of myopia is typically at approximately eight years of age and progresses until 15 or 16 years of age.
Myopia is the result of the eyes growing longer than normal, and the longer the eye becomes, the higher the degree of myopia.
Girls are at higher risk, as are children living in urban environments.
Urban settings, have more opportunities for educational advancement, which may lead to increase near work, activities, and urban dwellers have limited access to outdoor activities compared with those in rural areas.
Spending time outdoors may help prevent myopia development or at least delay its onset.
It is recommended that children spend between one and two hours outside each day.
Outdoors has the highest level of evidence as the environmental influence that has the most effect on refractive error.
Outdoor lighting is 100 times brighter than being indoors and stimulates the eye with light that is more varied and requires different eye movements and focus than when inside.
There is a connection between when children start education and the occurrence of myopia, as earlier schooling is associated with increased prevalence of myopia.
Asia has the highest estimated prevalence of childhood myopia at 35%, led by Japan at 86% and South Korea 74%.
Latin America and the Caribbean have the lowest rate at less than 4%.
Progression of myopia during that age group can slowed with soft multifocal contact lenses, orthokeratology contact lenses, and low concentration atropine.
It is associated with sight threatening ocular sequelae: cataracts, retinal detachment, glaucoma, and choroidal atrophy.
It is estimated to affect 50 percent of the world’s population by 2050.
The exact mechanisms of myopic eye growth and its progression remain unknown.
Among preschool children in US <6% have myopia with increasing prevalence with age.
Severe myopia associated with increased risk of retinal detachment, glaucoma, and cataract.
Increasing prevalence worldwide.
Increased prevalence in Asia.
In Asia myopia approaches nearly 40%, with higher rates among more educated and older students.
Associated with lower quality of life, especially with higher degree of myopia.
Can lead to retinal detachment, and myopic macular degeneration.
Severe myopia, refractive error worse than -6 diopters.
No effective preventive intervention.
Slowing myopic progression by using corrective lenses has limited success.
The age at which a child first develops myopia is the best predictor of the final magnitude of this problem as an adult.
Therefore delaying the onset of myopia has the potential to reduce how myopic the person becomes
Low dose atropine eyedrops shows promise in preventing preventing myopia.
Study suggests addition of outdoor activity daily compared with usual activity reduces the incidence of myopia (Mingguang-He et al).
There is a 9.3 fold increase in odds of having myopia among a group of adolescent male students from an ultraOrthodox community exposed to intense near-work activities from a very young age compared with aged matched secular adolescent male students without this exposure (Bez).
Among children with myopia treatment with high add power multifocal contact lenses compared with medium add power multifocal and single vision contact lenses reduces the rate of myopia progression over three years (Walline JJ).
Delaying the onset of myopia allows children a longer time with correction free, clear vision.
Multifocal optical corrections and low-dose atropine drops are available to slow my progression rate as long as the eye is still growing: neither show significant improvement, however.